
The phrase "peptides for healing" gets used loosely. It covers everything from gut ulcers to torn rotator cuffs to post-laser skin. The biology underneath is more specific. This guide separates the four peptides with the strongest preclinical signal, what each one actually does at the cellular level, and where the evidence stops.
Key takeaways#
- BPC-157, TB-500, GHK-Cu, and KPV target distinct phases of repair: angiogenesis, cell migration, matrix synthesis, and inflammation control.
- BPC-157 has a very short half-life (less than 30 min) yet its angiogenic, anti-inflammatory, and tissue regeneration effects appear to persist for weeks to months in animal studies.
- Thymosin beta-4 (the parent of TB-500) increased reepithelialization by 42% over saline controls at 4 days and as much as 61% at 7 days post-wounding in a rat full-thickness wound model.
- GHK levels in human serum average 200 ng/ml at age 20 but decline to roughly 80 ng/ml by age 60, which is why exogenous GHK-Cu is studied for age-related repair deficits.
- KPV is a three-amino-acid fragment of alpha-MSH that down-regulates NF-κB signalling, the master switch for inflammatory gene expression.
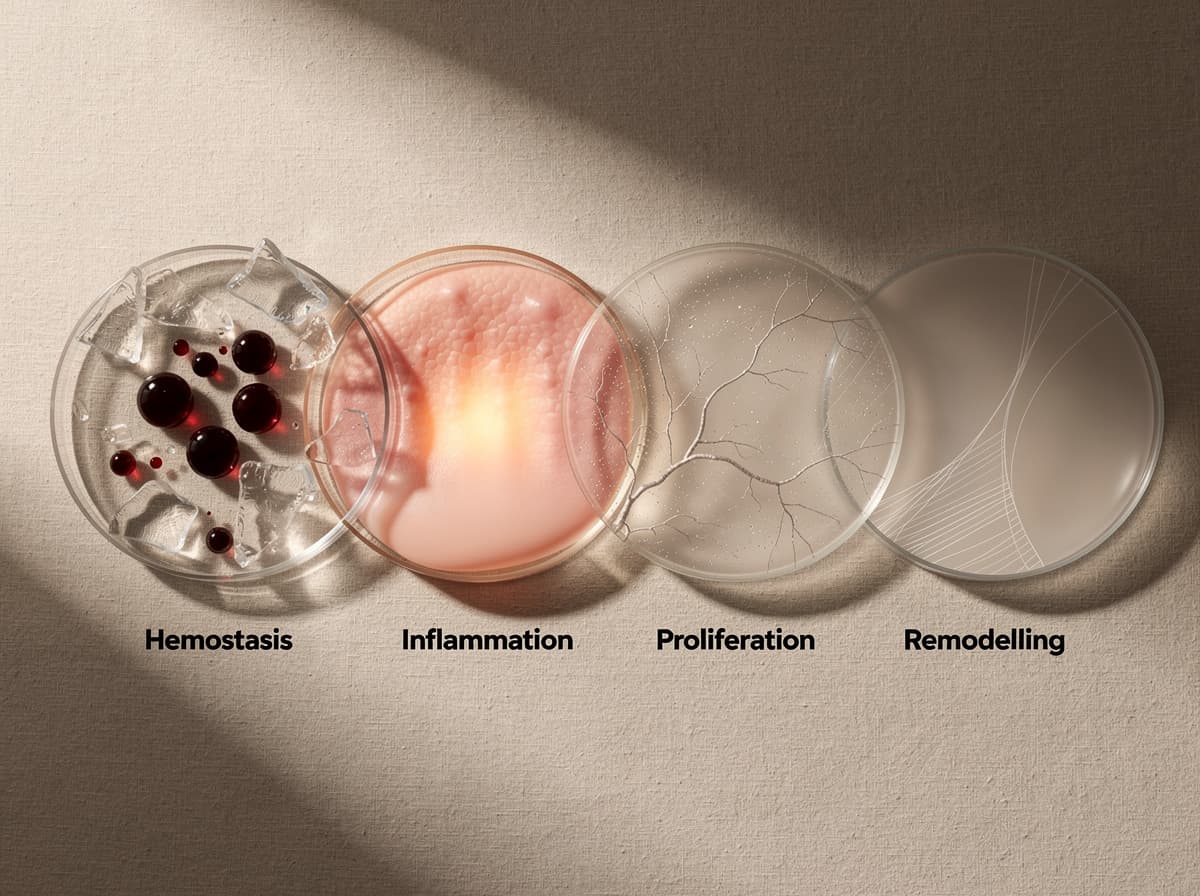
Healing is four phases, not one#
Tissue repair is not a single event. It is hemostasis, inflammation, proliferation, and remodelling, each with its own dominant cell types and signalling molecules. A peptide that accelerates one phase may do nothing for another. This is why a "stack" question usually has a phase-specific answer.
BPC-157 and TB-500 act mostly during proliferation, when fibroblasts and endothelial cells need to migrate into the wound bed. GHK-Cu spans proliferation and remodelling, modulating collagen turnover and angiogenesis. KPV intervenes earlier, dampening the inflammatory phase before it becomes destructive. Understanding which peptide fits which phase is the difference between a coherent protocol and a shopping list.
BPC-157 has been shown to accelerate tendon, ligament, and muscle repair in animal models#
BPC-157 is a 15-amino-acid sequence derived from a protein found in human gastric juice. The preclinical record for soft-tissue healing is unusually consistent across labs. Tested at days 1, 4, 7, 10, 14, and 21 after Achilles detachment, BPC 157 improves healing functionally (Achilles functional index values substantially increased), biomechanically (load to failure, stiffness, and Young elasticity modulus significantly increased), macro- and microscopically, and immunohistochemically with better organisation of collagen fibres and more collagen type I.
The mechanism is multi-pathway. BPC 157 significantly accelerated the outgrowth of tendon explants. Cell proliferation of cultured tendon fibroblasts was not directly affected as evaluated by MTT assay. However, the survival of BPC 157-treated cells was significantly increased under H2O2 stress, and BPC 157 markedly increased the in vitro migration of tendon fibroblasts in a dose-dependent manner. Translation: it does not just push cells to divide faster, it keeps them alive under oxidative stress and helps them move to where they are needed. Research suggests this is closer to what injured tissue actually requires.
Effects extend beyond tendon. Studies have shown that BPC 157 improved muscle healing in crushed rats, macroscopically (less hematoma and edema, no post-injury leg contracture), microscopically, functionally, and based on enzyme activity, accelerating post-injury muscle healing and helping to restore full function. A 2025 narrative review concluded that preclinical studies consistently highlight BPC-157's ability to accelerate tendon, muscle, and ligament healing, even under compromised conditions, and its proposed mechanisms (from nitric oxide modulation to neuromuscular junction stabilisation) suggest it may significantly enhance recovery and functional outcomes in musculoskeletal injuries.
The honest caveat: human RCT data is still thin. The signal is preclinical, not phase-3.
TB-500 mobilises cells to the injury site through actin regulation#
TB-500 is a synthetic version of the active region of thymosin beta-4 (Tβ4), a protein released by platelets and macrophages after injury. Tβ4 is a low molecular weight, naturally-occurring peptide that plays a vital role in the repair and regeneration of injured cells and tissues. After injury, it is released by platelets, macrophages and many other cell types to protect cells and tissues from further damage and reduce apoptosis, inflammation and microbial growth. It binds to actin and promotes cell migration, including the mobilisation, migration, and differentiation of stem and progenitor cells, which form new blood vessels and regenerate tissue. It also decreases the number of myofibroblasts in wounds, resulting in decreased scar formation and fibrosis.
The wound-healing effect size in animal models is notable. Addition of Tβ4 topically or intraperitoneally increased reepithelialisation by 42% over saline controls at 4 days and as much as 61% at 7 days post-wounding. Treated wounds also contracted at least 11% more than controls by day 7. Increased collagen deposition and angiogenesis were observed in the treated wounds. Ligament data is similar: in healing femur-medial collateral ligament-tibia complexes, the Tβ4-treated group had significantly better biomechanical properties than the control group at 4 weeks after surgery, and local administration of Tβ4 promotes the healing process of MCL, both histologically and mechanically, in a rat model.
What ties these effects together is systemic action. Once injected, TB-500 circulates and concentrates at sites of active injury, which is associated with effects observed at injury sites distant from the injection point. The human evidence base is more limited than the animal data, with some early trials of full thymosin beta-4 in dry eye disease and chronic wounds.
GHK-Cu drives collagen synthesis, angiogenesis, and antioxidant defence in skin#
GHK is a tripeptide (glycyl-L-histidyl-L-lysine) that complexes naturally with copper. It is the most studied repair peptide in dermatology. GHK is present in human plasma, saliva, and urine but declines with age. It functions as a complex with copper 2+ which accelerates wound healing and skin repair. GHK stimulates both synthesis and breakdown of collagen and glycosaminoglycans and modulates the activity of both metalloproteinases and their inhibitors. It stimulates collagen, dermatan sulfate, chondroitin sulfate, and the small proteoglycan, decorin.
The collagen response is dose-dependent and large. In a rat wound chamber model, GHK-Cu injections significantly increased the collagen content of the wound chambers at days 18 and 22 (396% and 538% of the corresponding controls, respectively, p < 0.05). Glycosaminoglycan accumulation followed a similar curve. Research has shown that wound healing activity of GHK-Cu was confirmed in animal experiments. GHK-Cu accelerated wound healing and increased blood vessel formation and antioxidant enzyme levels in rabbits. It also induced systemic wound healing in rats, mice, and pigs and improved the healing of diabetic and ischemic wounds in rats, decreasing TNF-alpha and stimulating collagen synthesis.
The angiogenic mechanism is well-characterised. GHK-Cu at 1 nM increases bFGF and VEGF expression in irradiated human dermal fibroblasts, both of which aid blood vessel formation and blood flow into damaged tissues. It also increases HUVEC proliferation by stimulating VEGF and FGF-2 expressions, and at low concentrations is a powerful attractant for capillary cells that build new blood vessels and a migration stimulant for macrophages and mast cells that remove damaged cellular debris.
Clinical context matters. GHK-Cu has been used in cosmeceutical formulations for decades, with topical research showing improvements in fine lines and skin density. The peptide has also been studied as an adjunct after CO2 laser resurfacing, with patient-reported satisfaction outcomes favouring the GHK-Cu regimen even when blinded erythema scoring did not separate the groups.
KPV controls the inflammation that delays repair#
If BPC-157 and TB-500 push cells forward, KPV pulls inflammation back. KPV (Lys-Pro-Val) is the C-terminal tripeptide of alpha-MSH and retains most of the parent molecule's anti-inflammatory activity at a fraction of the size. Most of the anti-inflammatory activities of α-MSH can be attributed to its C-terminal tripeptide KPV. K(D)PT, a derivative of KPV, is currently emerging as another tripeptide with potent anti-inflammatory effects. The anti-inflammatory potential together with favourable physicochemical properties most likely will allow these agents to be developed for the treatment of inflammatory skin, eye and bowel diseases, allergic asthma and arthritis.
The mechanism centres on NF-κB, the transcription factor that activates most pro-inflammatory genes. An important molecular mechanism underlying the anti-inflammatory effects of α-MSH, such as modulation of pro-inflammatory cytokine and adhesion molecule expression, appears to be the suppression of nuclear factor-κB (NF-κB) activation. Preliminary evidence in colonic models supports oral activity: nanomolar concentrations of KPV inhibit the activation of NF-κB and MAP kinase inflammatory signaling pathways and reduce pro-inflammatory cytokine secretion. KPV acts via hPepT1 expressed in immune and intestinal epithelial cells. Oral administration of KPV reduces the incidence of DSS- and TNBS-induced colitis indicated by a decrease in pro-inflammatory cytokine expression. This study indicates that KPV is transported into cells by PepT1 and might be a new therapeutic agent for IBD.
Research has shown that the effect is associated with both gut and airway tissue. In bronchial epithelium, KPV and γMSH evoked a dose-dependent inhibition of NF-κB, matrix metalloproteinase-9 activity, IL8 and eotaxin secretion. The implication: KPV is positioned for situations where chronic, low-grade inflammation is itself the obstacle to healing, gut barrier dysfunction, post-procedure skin reactivity, and similar contexts.
Stacking logic: pair phases, do not duplicate them#
The most common combination in the wellness literature is BPC-157 plus TB-500. The rationale is mechanistic, not just additive. BPC-157 increases fibroblast survival and migration. TB-500 mobilises stem and progenitor cells systemically and improves angiogenesis. Run together, the two cover proliferation more comprehensively than either alone.
GHK-Cu sits downstream, optimising the matrix that the migrating cells produce. Topical GHK-Cu after a skin injury or laser procedure is a different intervention from injected BPC-157 for a tendon, even though both fall under "peptides for healing". KPV, by contrast, is the brake. It is most relevant when inflammation is the bottleneck, not when proliferation is.
Klarovel's peptide calculator maps these phase relationships to dose-equivalent reconstitution, so the protocol layer is consistent across compounds. Klarovel curates the protocol logic only; it does not sell, source, or fulfil peptides.
What the evidence does not yet show#
The honest summary: most of what is known about peptides for healing comes from animal models, in vitro work, and small clinical series. Large randomised controlled trials in humans are limited for all four compounds discussed. These findings support the rationale for initiating formal human clinical trials. BPC-157 demonstrates therapeutic potential across a broad range of musculoskeletal injuries through its angiogenic, anti-inflammatory, cytoprotective, and tissue-regenerative properties. The word "potential" is doing real work in that sentence.
Regulatory status reflects this. None of these peptides are approved as medicines for healing indications by the FDA, EMA, or Legemiddelverket. They sit in research-use-only or compounding-pharmacy frameworks depending on jurisdiction, and that classification can change. Anyone considering use should track current regulatory positions and work under qualified supervision.
Read more on Klarovel#
- BPC-157 peptide: mechanism, evidence, and protocol guide: BPC-157 is the most-searched healing peptide.
- BPC-157 + TB-500 stack: what the evidence actually says: The BPC-157 + TB-500 stack is the most common healing peptide protocol.
- BPC-157 vs GHK-Cu: which tissue-repair peptide wins in 2026?: BPC-157 vs GHK-Cu compared on mechanism, dosing, evidence and side-effect profile.
- BPC-157 vs TB-500: when to use each for tissue repair: BPC-157 and TB-500 are the two most-researched tissue-repair peptides.
- GHK-Cu copper peptide: skin and hair research review: GHK-Cu is the fastest-growing peptide in search volume.
- KPV peptide guide: what the preclinical research shows: KPV is the three-amino-acid fragment of alpha-MSH.
- TB-500 (thymosin beta-4): mechanism and protocol guide: TB-500 is the synthetic thymosin beta-4 fragment used in tissue-repair research.
- Wolverine peptide stack: definition, doses and duration: The Wolverine peptide stack means BPC-157 plus TB-500.
Build the protocol before you build the stack#
Peptides for healing are not a category of supplement. They are a set of biochemically distinct tools that map onto specific phases of tissue repair. The interesting question is not "which peptide is strongest" but "which phase is currently rate-limiting for this injury, in this person, at this point in recovery". Answer that, and the stack writes itself. Register with Klarovel to access the protocol layer, the phase-mapped calculator, and the tracking tools that turn a peptide list into a research-grade plan.
Frequently asked questions
Keep reading
Hexarelin Peptide: The Forgotten GHRP and Why It Faded
Hexarelin was once the most potent GHRP known. Research suggests tachyphylaxis and CD36 side effects explain why the peptide world moved on.

Tesofensine: The Fourth-Class Weight Loss Peptide Guide
Tesofensine is a triple monoamine reuptake inhibitor that produced 10.6% weight loss in Phase 2. Mechanism, doses, safety, and GLP-1 comparison.

Peptides for Bodybuilding: What the GH-Axis Research Shows
A clinical look at GH-axis peptides used in physique work: what the human trials on MK-677, CJC-1295 and ipamorelin actually document, plus WADA rules.