PT-141 sits in an unusual corner of sexual health pharmacology. It does not relax blood vessels, it does not raise testosterone, and it does not act on the genitals at all. Instead it engages receptors in the brain that govern the upstream signal of desire itself, which is why the conversation around it looks so different from the one around sildenafil or tadalafil.
Key takeaways#
- PT-141 (bremelanotide) is a cyclic heptapeptide and melanocortin receptor agonist, primarily active at MC3R and MC4R in the hypothalamus.
- It received FDA approval in June 2019 as Vyleesi for premenopausal women with acquired, generalized hypoactive sexual desire disorder (HSDD).
- The standard labeled dose is 1.75 mg subcutaneous, taken roughly 45 minutes before anticipated sexual activity, with a hard cap of one dose per 24 hours and eight doses per month.
- The RECONNECT phase 3 trials (n = 1,247 safety population) showed statistically significant gains in the FSFI-desire domain and reductions in distress versus placebo.
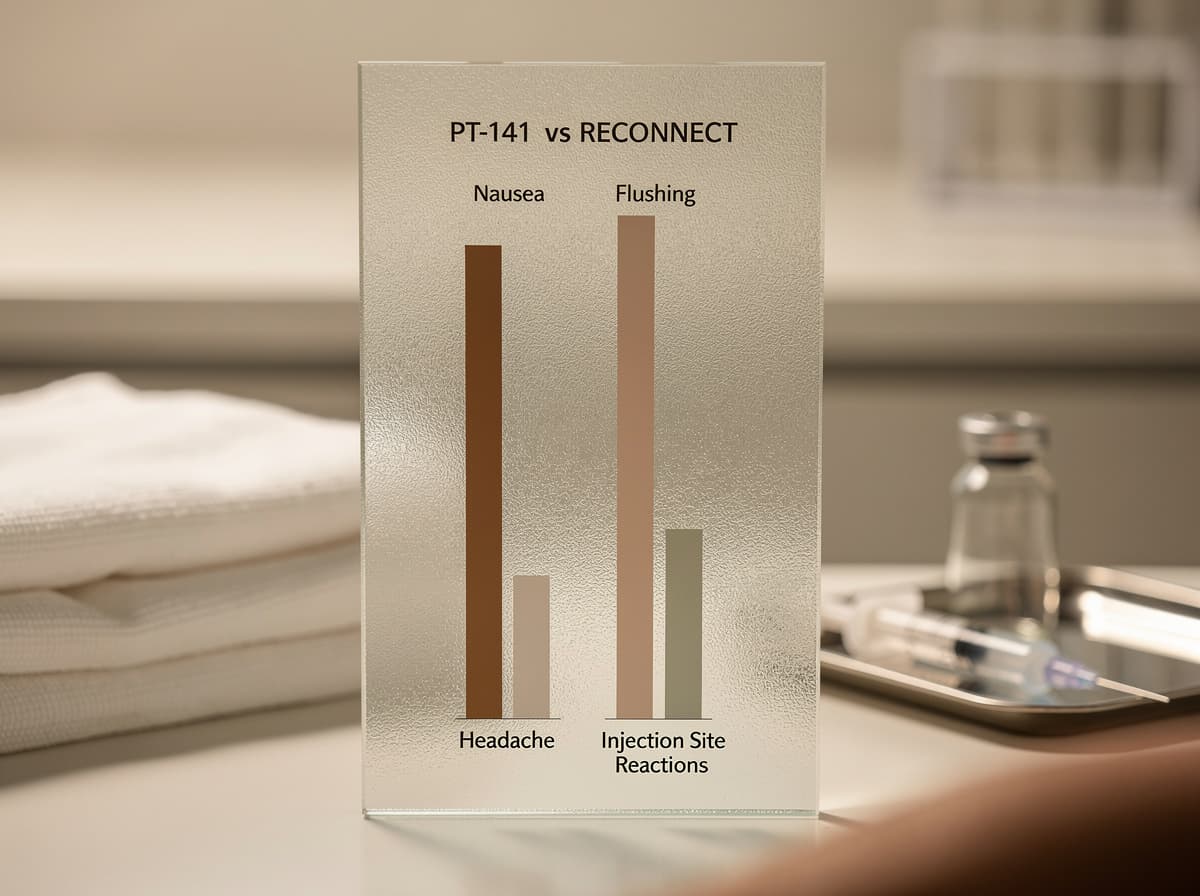
- Nausea affects roughly 40% of users, flushing about 20%, and transient blood pressure elevation is a documented effect; uncontrolled hypertension is a contraindication.
PT-141 acts on the brain, not the bloodstream#
The mechanism is what separates PT-141 from every other compound marketed for sexual function. Unlike phosphodiesterase type 5 inhibitors, which act peripherally by enhancing vascular smooth muscle relaxation, PT-141 acts centrally, engaging melanocortin receptors in the brain to influence the neurological and hormonal substrates of sexual response.
Structurally, PT-141, chemically designated as bremelanotide, is a cyclic heptapeptide analog of alpha-melanocyte-stimulating hormone (α-MSH) that acts as a non-selective melanocortin receptor agonist. The cyclization is not cosmetic chemistry. The cyclic structure creates a constrained three-dimensional shape that fits melanocortin receptor binding pockets with high affinity, particularly MC4R. This conformational constraint also provides resistance to enzymatic degradation, extending its functional half-life relative to linear analogs.
Of the five melanocortin receptor subtypes, two carry most of the sexual-function signal. PT-141 demonstrates activity at multiple melanocortin receptor subtypes but is primarily studied for its effects mediated through MC3R and MC4R, the receptor subtypes most highly expressed in the hypothalamus and limbic system. MC4R is of particular research interest in the context of sexual function. Downstream, activation of adenylyl cyclase and cyclic adenosine monophosphate (cAMP) signaling pathways and enhanced oxytocin and dopamine release in reward pathways are how the receptor binding translates into a subjective shift in desire.
This is the practical implication: PT-141 is not a fallback for PDE5 non-responders in the sense of "another tool that does the same thing." It works on an entirely upstream node. Research has shown that the compound's effects persist in models where PDE5 inhibitors are ineffective, which is consistent with a distinct neural pathway rather than a redundant vascular one.
From Melanotan II to Vyleesi: how PT-141 reached the clinic#
The peptide's origin story explains a few of its quirks, including the pigmentation question. PT-141 emerged from research initially conducted on Melanotan II (MT-II), a non-selective melanocortin receptor agonist developed in the 1980s. During clinical testing of MT-II, researchers observed unexpected and consistent pro-erectile effects in male participants, prompting further investigation into the melanocortin pathway as a therapeutic target for sexual dysfunction. Bremelanotide was subsequently developed as a more selective and clinically refined compound.
Regulatory history is concrete. According to the FDA Vyleesi label, Vyleesi is a melanocortin receptor agonist indicated for the treatment of premenopausal women with acquired, generalized hypoactive sexual desire disorder (HSDD) , with initial U.S. approval granted in 2019. Palatin Technologies confirmed the date in its press release, and the approval letter on FDA's site lists June 21, 2019.
The label defines its scope narrowly. Contraindications include uncontrolled hypertension or known cardiovascular disease. Warnings cover transient increase in blood pressure and decrease in heart rate. The FDA explicitly states that Vyleesi is not indicated for treatment of HSDD in postmenopausal women or in men and is not indicated to enhance sexual performance.
That last sentence is important for honest framing. Off-label use in men and in postmenopausal women does happen, and some clinical literature exists around it, but it sits outside the approved indication and outside the population studied in the registration trials.
What the RECONNECT trials actually showed#
The efficacy evidence rests on two large phase 3 trials. As reported in Obstetrics & Gynecology, two identical phase 3, randomized, double-blind, placebo-controlled, multicenter clinical trials (RECONNECT) evaluated the safety and efficacy of bremelanotide 1.75 mg administered subcutaneously as needed in premenopausal women with hypoactive sexual desire disorder. Patients were randomized 1:1 to 24 weeks of treatment with bremelanotide or placebo. The trials enrolled 1,267 women randomized, 1,247 and 1,202 in the safety and efficacy (modified intent-to-treat) populations, respectively.
The numbers behind the approval were modest but consistent. Studies have shown that relative to those in the placebo group, women in the bremelanotide group had statistically significant increases in sexual desire from baseline to end of study, as measured by FSFI-D scores (study 301: 0.30, P less than .001; study 302: 0.42, P less than .001; integrated studies 0.35, P less than .001) and statistically significant reductions in distress related to low sexual desire, as measured by FSDS-DAO scores (study 301: -0.37, P less than .001; study 302: -0.29, P = .005; integrated studies -0.33, P less than .001) compared with placebo.
Those are real effects, but they are not transformative on a per-person basis. The FSFI-desire scale runs from 1.2 to 6.0, and a mean change of 0.35 sits in the small-to-moderate effect-size range. The clinically meaningful piece is that distress dropped alongside desire, which is the criterion that distinguishes HSDD from ordinary fluctuations in libido.
Qualitative data backed the numbers. Research has shown that participants who received bremelanotide described increased feelings of sexual desire, physical arousal, and improvements in overall quality of their sexual activities in their partner relationship.
Dosing: the labeled protocol and why the limits exist#
The dosing is narrow and the rationale for each constraint is mechanistic. According to the PMC clinical review, the recommended dosage of bremelanotide is 1.75 mg injected subcutaneously in the abdomen or thigh at least 45 min before sexual activity.
The frequency cap is not arbitrary. Preliminary evidence and post-marketing data both point to dose-cumulative effects. The FDA-approved labeling recommends limiting PT-141 use to no more than 8 doses per month for several reasons: blood pressure effects. PT-141 temporarily increases blood pressure (systolic BP may rise 6 to 8 mmHg for 6 to 12 hours post-dose). Frequent use could contribute to sustained BP elevation. The second reason is pigmentation. A dose-dependent side effect of melanocortin agonism is skin darkening (hyperpigmentation), particularly of the face, gums, and breasts. This effect is cumulative and more pronounced with higher frequency of use.
For anyone planning a session schedule, the Klarovel peptide calculator can help map the labeled 1.75 mg dose against reconstitution volume and injection planning. The point of dose discipline here is not over-caution; it is that the safety profile genuinely degrades with frequency in ways that show up on physical exams.
Side effects: what users actually experience#
The side-effect profile is dominated by gastrointestinal and vasomotor symptoms. The contemporary OB/GYN summary of RECONNECT reports that patients who took bremelanotide experienced higher rates of nausea (40.0% compared with 1.3% placebo), flushing (20.3% compared with 0.3% placebo), and headache (11.3% compared with 1.9% placebo).
The nausea has a mechanistic explanation. Research suggests the nausea is likely mediated by melanocortin receptor activation in the area postrema (the chemoreceptor trigger zone), a brain region involved in nausea and vomiting that lies outside the blood-brain barrier and is accessible to circulating peptides. This is also why nausea typically attenuates after the first one or two doses but rarely disappears entirely.
The pigmentation question is more nuanced than internet summaries usually capture. The melanocortin family directly drives melanogenesis, so any MC1R activity carries a pigmentation signal. The hyperpigmentation may develop gradually with repeated use and can be persistent after discontinuation. The mechanism is stimulation of melanogenesis through MC1R activation in melanocytes. While reduced compared to Melanotan-2, PT-141 retains sufficient MC1R activity to cause pigmentation changes in susceptible individuals. In the registration trials, hyperpigmentation was associated with a small minority of users, but the risk concentrates in people who exceed the monthly dose cap.
Cardiovascular monitoring is the non-negotiable piece. The FDA label requires uncontrolled hypertension as an exclusion, and any program of repeat use should include baseline and follow-up blood pressure measurement. This is also why partner-supplied compounded versions, sometimes sold as intranasal sprays, deserve scrutiny: the dose-response on blood pressure is real even when the route changes.
Where PT-141 fits versus PDE5 inhibitors and hormonal options#
The pragmatic question for most people is not "does PT-141 work" but "does it work for what I'm dealing with." Because the compound targets desire and central arousal rather than erectile mechanics or vaginal tissue, it occupies a different slot in the toolkit.
For erectile dysfunction with intact desire, PDE5 inhibitors remain first-line and far better evidenced. For low desire with adequate mechanical function, PT-141 has the mechanistic case and the regulatory imprimatur (in premenopausal women). For mixed presentations, the literature is sparser. Comparative work has shown that the central and peripheral pathways are dissociable and that compounds isolating CNS contributions behave differently from PDE5 agents.
Hormonal causes deserve to be ruled out first. Low testosterone in men, thyroid dysfunction, hyperprolactinemia, and SSRI-induced sexual side effects can all present as low desire and none of them are addressed by PT-141. A peptide that engages a downstream neural circuit cannot correct an upstream endocrine deficit. The Klarovel methodology page walks through how the protocol layer weights these baseline checks before any peptide consideration enters the picture.
The honest read on PT-141#
PT-141 is the only compound on the market that addresses sexual desire through a confirmed central neural mechanism, and that alone makes it scientifically interesting. The effect size in trials is real but modest, the side-effect profile is manageable but not trivial, and the labeled indication is narrower than most consumer-facing summaries suggest. It is not a fix for low testosterone, relationship dynamics, SSRI side effects, or postmenopausal hormonal change, and it is not approved for men. Used inside its labeled scope, with attention to blood pressure and dose frequency, it offers something that the rest of the sexual-health toolkit does not: a way to engage the upstream signal rather than the downstream plumbing. To build a protocol around evidence rather than marketing, create a Klarovel account and walk through the methodology behind every peptide recommendation in our disclosures.
Frequently asked questions
Keep reading

Sermorelin: A Complete Guide to the GHRH 1-29 Analog
Sermorelin is a 29-amino-acid GHRH analog with a short half-life and long-tail GH effect. Here is what the primary literature actually shows in adults.
Peptides for Longevity: the 2026 Evidence Map
A pillar guide to peptides studied for longevity: NAD+, MOTS-c, Epitalon, SS-31. Mechanisms, evidence quality, and where the human data still sits in 2026.
Cerebrolysin: Complete Guide to the Neuropeptide Mixture
An evidence-based look at Cerebrolysin: porcine-derived neuropeptides, trial data across stroke, dementia and TBI, dosing protocols, and safety signals.