Thymosin alpha-1 sits in an unusual position in the peptide landscape. It is one of the most extensively studied research peptides in existence, yet outside of chronic viral hepatitis its evidence base is genuinely mixed. This guide separates the well-supported mechanistic biology from the indications where the data is still maturing.
Key takeaways#
- Thymosin alpha-1 (Tα1, brand name thymalfasin or Zadaxin) is a 28-amino-acid thymic peptide identical in sequence to the human endogenous form, with a reference subcutaneous dose of 1.6 mg twice weekly used in chronic hepatitis B registration trials.
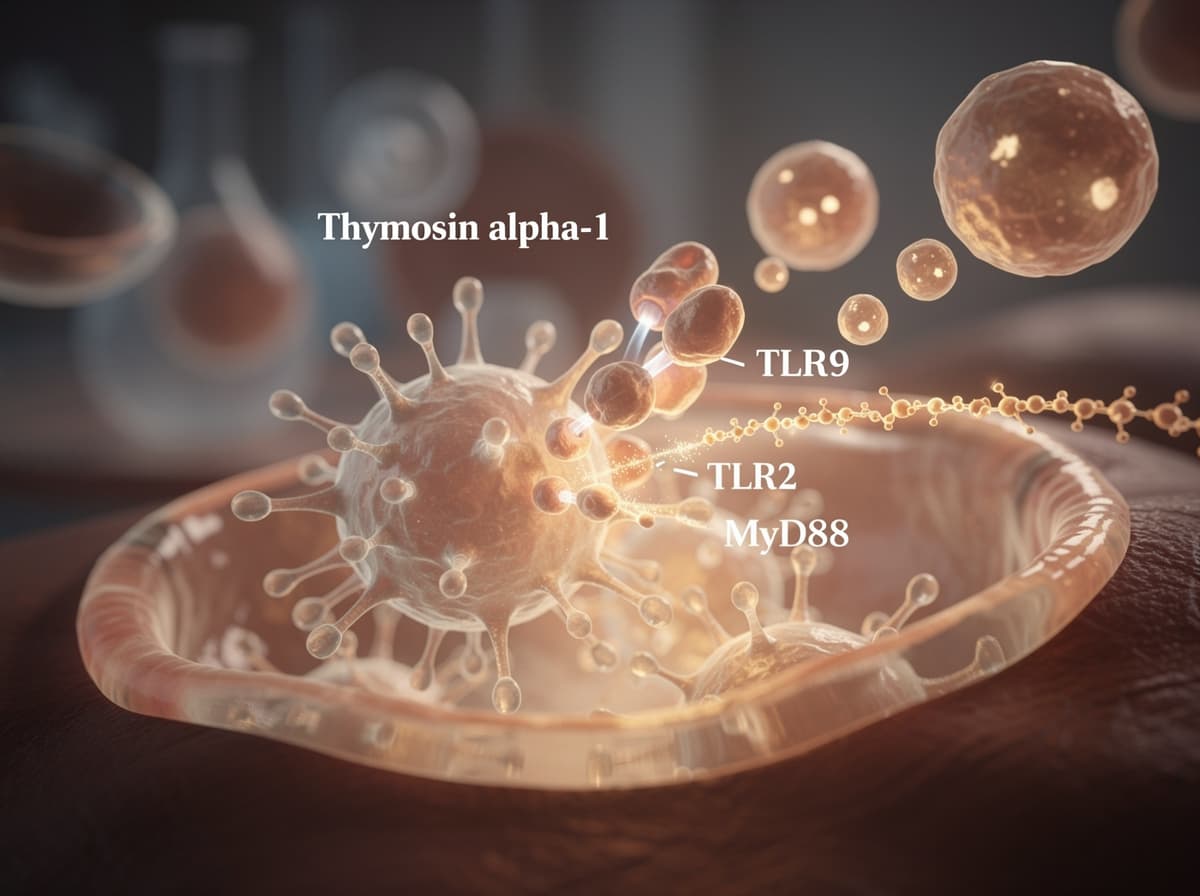
- Its mechanism is receptor-defined: it engages Toll-like receptors (chiefly TLR2 and TLR9) on dendritic cells, triggering MyD88-dependent signaling and downstream T-cell and NK-cell activation.
- The largest sepsis trial to date (TESTS, phase 3, published 2025) did not meet its primary mortality endpoint overall, although prespecified subgroups showed signal in older and diabetic patients.
- More than 11,000 subjects across over 30 clinical trials and post-marketing data covering over 600,000 patients underpin a benign tolerability profile, with injection-site reactions and transient flu-like symptoms the most common adverse events.
- The peptide has a short plasma half-life (around 2 hours), which informs the twice-weekly chronic regimen and the every-12-hour acute dosing patterns used in critical illness research.
A 28-amino-acid thymic peptide with a defined molecular target#
Thymosin alpha-1 was the first individual peptide isolated from the thymic fraction that retained immunological activity. Tα1, brand name Zadaxin and INN thymalfasin, is a small molecule polypeptide with 28 amino acids at about 3.1 kDa . The synthetic form used in research and registered products is chemically identical to the endogenous peptide.
Its mechanism is unusually well characterised for an immunomodulatory peptide. Tα1 acts through Toll-like receptors (TLR2 and TLR9) in myeloid and plasmacytoid dendritic cells, leading to the activation and differentiation of dendritic cells and T cells, as well as the initiation of cytokines such as interferon-gamma and interleukin-2 . Research has shown that the same peptide also engages TLR3, TLR4, and TLR7 pathways depending on cell context, with TLR2/NF-κB, TLR2/p38MAPK, and TLR7/MyD88 cascades feeding into innate and adaptive cytokine production.
The practical consequence is that Tα1 is not a single-axis stimulator. Studies have shown it bridges innate sensing (the dendritic cell compartment) with adaptive maturation (T-cell priming), which is why its strongest preclinical signal is in settings where both arms are compromised: chronic viral infection, post-chemotherapy immune injury, and sepsis-associated immune paralysis.
The hepatitis B reference dose anchors everything else#
The dosing pattern that defines thymalfasin comes from its chronic hepatitis B registration program. The recommended dose of Zadaxin for chronic hepatitis B, used as monotherapy or with interferon, is 1.6 mg (900 µg/m²) administered subcutaneously twice a week for 6 to 12 months. Patients weighing less than 40 kg should receive a dose of 40 µg/kg. The peptide is supplied as a lyophilized 1.6 mg vial with mannitol and sodium phosphate buffer, reconstituted with sterile water immediately before subcutaneous injection.
Pharmacokinetics constrain the schedule. Thymalfasin has a short elimination half-life of approximately 2 hours, and this rapid clearance means the drug does not accumulate with repeated dosing such as the twice-weekly regimen used for chronic indications. That short half-life is also why acute critical-illness research has tested far more frequent dosing rather than higher single doses.
Across the broader literature, common research dosing is 1.6 mg given twice weekly or daily, with durations from one to eight weeks depending on the trial. The 1.6 mg unit dose is essentially the only one validated in registration data; deviations are unvalidated.
What the chronic hepatitis B data actually shows#
Hepatitis B is where the evidence is strongest. The registered indication rests on pooled randomized data: Zadaxin is indicated for chronic hepatitis B in patients 18 and older with compensated liver disease and HBV replication, based on a pooled analysis of 3 randomized controlled trials comprising 223 patients, with twice-weekly dosing for 6 months and follow-up at 12 months, and a notable delayed therapeutic response 12 months or longer after completion of therapy.
The delayed-response pattern matters. Unlike direct-acting antivirals where viral suppression tracks dosing, Tα1's effect on HBV markers tends to manifest after the dosing course ends, consistent with an immune-reconstitution mechanism rather than a direct antiviral one. This is associated with the peptide's role as a dendritic cell maturation signal rather than a viral enzyme inhibitor.
Preliminary evidence in hepatitis C and as a vaccine adjuvant follows the same pattern: modest but real signal when the underlying problem is immune insufficiency, weak or null signal when the host immune system is already competent.
The sepsis story is more complicated than the early signal suggested#
Sepsis is the indication where the gap between preliminary enthusiasm and confirmatory data is widest. The early ETASS trial (2013) was encouraging: eligible patients admitted to ICU with severe sepsis were randomly allocated to control or Tα1 (1:1 ratio), with death from any cause assessed 28 days after enrollment as the primary outcome . ETASS reported a reduction in 28-day mortality and was followed by a series of smaller meta-analyses suggesting benefit.
The definitive test was the phase 3 TESTS trial, published in 2025. Its findings tempered expectations. According to the TESTS trial report, the prespecified subgroup analysis showed a potential differential effect on the primary outcome based on age (under 60 years: hazard ratio 1.67, 1.04 to 2.67; 60 years or older: 0.81, 0.61 to 1.09; P for interaction equals 0.01) and on diabetes (diabetes: 0.58, 0.35 to 0.99; no diabetes: 1.16, 0.87 to 1.53; P for interaction equals 0.04).
In plain language: the overall primary endpoint was not clearly met, but older patients and diabetic patients appeared to benefit, while younger non-diabetic patients may have done worse. A more recent 2025 systematic review and meta-analysis pooled the broader literature and reported that Tα1 therapy was associated with reduced 28-day mortality (OR 0.73, 95% CI 0.59 to 0.90, P equals 0.003), but the TESTS subgroup heterogeneity is a real caution and not a footnote.
COVID-19: a worked example of why retrospective data oversells#
Tα1 was used widely in China during the early COVID-19 waves, and the retrospective signal was striking. One Wuhan cohort reported that hospitalized patients receiving Tα1 showed improved lymphocyte subsets and a reduction in mortality from 30 to 11 percent (p equals 0.04).
But subsequent analyses complicated the picture. A Frontiers in Immunology study of 275 patients found no beneficial effect of Tα1 on restoring CD4+ and CD8+ T lymphocyte counts. A propensity-score-matched cohort of 1,388 non-severe patients found that the proportion progressing to severe COVID-19 was 2.17 percent for the Tα1 group versus 2.71 percent for controls (p equals 0.736), with no significant mortality difference, though duration of viral shedding and hospital stay were shorter in the Tα1 group. The pattern across the COVID-19 literature is the pattern across the broader Tα1 literature: signal in immune-compromised hosts, noise in immune-competent ones.

Safety, dosing patterns, and what the catalog actually validates#
The safety record is one of the most reassuring features of the peptide. Post-marketing experience covers more than 600,000 patients, with Tα1 administered to elderly subjects up to 101 years old, children as young as 13 months, and immunocompromised patients; the most common adverse events in clinical trials have been mild injection-site pain lasting under 30 minutes, plus mild-to-moderate fever, nausea, and flu-like symptoms. No dose-limiting toxicities or organ injury have been associated with the standard regimen.
For researchers calculating doses, the Klarovel peptide calculator handles the reconstitution math for the 1.6 mg vial and the common 5 mg or 10 mg research vials. Standard dosing patterns in the published literature include:
- Chronic hepatitis B reference: 1.6 mg subcutaneously twice weekly for 6 to 12 months.
- Sepsis investigational (TESTS protocol): 1.6 mg every 12 hours for seven days.
- Vaccine adjuvant research: shorter 2 to 4 week courses around vaccination.
- Cancer adjuvant investigational: 1.6 mg daily during chemotherapy cycles, twice weekly between cycles.
Each of these should be cross-checked against the Klarovel research catalog before any protocol work; the catalog reflects the dose ranges with supporting peer-reviewed evidence.
How thymosin alpha-1 compares to other immune peptides#
Tα1 is mechanistically distinct from the other peptides in the immune cluster. LL-37 is a direct antimicrobial peptide acting at the membrane level. Thymulin is a different thymic peptide acting on the zinc-dependent receptor axis. KPV is a small alpha-MSH fragment with anti-inflammatory rather than immune-priming actions. Tα1 is the one that hits TLR9 specifically, which makes it the candidate for settings where dendritic cell maturation is the rate-limiting step.
For deeper comparison work, see our how Klarovel evaluates peptide evidence framework, which weights primary endpoint outcomes in phase 3 trials more heavily than retrospective cohorts.
What this means for protocol decisions#
Thymosin alpha-1 has the cleanest mechanism story of any immune peptide in current research circulation and one of the strongest safety profiles. The clinical evidence base is uneven, strongest in chronic viral hepatitis, mixed in sepsis, and heterogeneous in COVID-19, but the underlying biology, TLR2 and TLR9 engagement on dendritic cells, is durable across the literature. For researchers building immune-axis protocols, Tα1 is a defensible choice when the indication is immune insufficiency rather than immune competence. Create a Klarovel account to access the dose calculator, the underlying citation catalog, and protocol templates aligned with the peer-reviewed evidence rather than the marketing narrative.
Frequently asked questions
Keep reading

Sermorelin: A Complete Guide to the GHRH 1-29 Analog
Sermorelin is a 29-amino-acid GHRH analog with a short half-life and long-tail GH effect. Here is what the primary literature actually shows in adults.
Peptides for Longevity: the 2026 Evidence Map
A pillar guide to peptides studied for longevity: NAD+, MOTS-c, Epitalon, SS-31. Mechanisms, evidence quality, and where the human data still sits in 2026.
Cerebrolysin: Complete Guide to the Neuropeptide Mixture
An evidence-based look at Cerebrolysin: porcine-derived neuropeptides, trial data across stroke, dementia and TBI, dosing protocols, and safety signals.