BPC-157 and KPV are the two oral-stable peptides researchers reach for when gut inflammation is the target. They share a route (oral works for both), they share a regulatory ceiling (both sit on the FDA's 2023 Category 2 list), and they share an evidence pattern that is deep in animals and thin in humans. What separates them is mechanism: BPC-157 is a broad cytoprotective and angiogenic agent that rebuilds tissue, while KPV is a focused transcription-factor inhibitor that quiets cytokine production. This guide decides which one fits which clinical picture.
Key takeaways#
- BPC-157 is a 15-amino-acid pentadecapeptide derived from gastric juice; KPV is the 3-amino-acid C-terminal fragment of α-MSH. They operate on completely different biological levels.
- BPC-157 is stable in human gastric juice for more than 24 hours and acts as a cytoprotective mediator that heals ulcers, wounds, and fistulas across the entire gastrointestinal tract, while KPV is transported into intestinal cells by PepT1 with a Km around 160 μM, among the lowest reported for this transporter.
- Research-published BPC-157 doses cluster at 250-500 mcg once or twice daily orally; KPV research protocols cluster at 200-500 mcg orally on an empty stomach.
- BPC-157 completed a Phase II ulcerative colitis trial as PL 14736, but results were never published in a peer-reviewed journal. KPV has no human IBD trials, only mouse colitis data.
- Both peptides sit on the FDA's September 2023 Category 2 list, meaning U.S. compounding pharmacies cannot prepare them; research-grade material is available from specialised suppliers.
How BPC-157 works#
BPC-157 is a synthetic pentadecapeptide (sequence GEPPPGKPADDAGLV) derived from a body protection compound originally isolated from human gastric juice. The defining feature is durability in the gut: it is native to and stable in human gastric juice for more than 24 hours , which is what makes oral administration plausible for a peptide of this size.
Mechanistically, BPC-157 does not bind a single receptor. Stimulated Egr-1 gene, NAB2, FAK-paxillin and JAK-2 pathways have been implicated in its tissue-repair effects. Research suggests it functions as a downstream amplifier of cytoprotection: angiogenesis, collateral vessel recruitment, growth-factor signalling, and nitric-oxide-system modulation. In rat fistula models, beneficial effects remained unchanged with blunted NO generation and with NO substrate , suggesting the peptide acts above the NO axis rather than through it.
The preclinical breadth is unusual. BPC-157 has been shown to support healing in stomach ulcers, colonic anastomoses, periodontitis, liver and pancreas lesions, tendon and ligament injuries, and corneal ulcers. It is effective in the whole gastrointestinal tract, and heals various wounds including skin, muscle, tendon, ligament, bone, ulcers in the entire gastrointestinal tract, and corneal ulcer; LD1 is not achieved . The route question is settled by the gastric-juice stability data: oral works.
How KPV works#
KPV is the carboxy-terminal tripeptide of α-melanocyte-stimulating hormone, sequence Lys-Pro-Val. Studies have shown that the minimum sequence required for anti-inflammatory activity of α-MSH is the C-terminal tripeptide Lys-Pro-Val . This is the interesting part: cutting the parent α-MSH down to three residues strips out the pigmentation, appetite, and arousal effects of melanocortin signalling while keeping the anti-inflammatory tail intact.
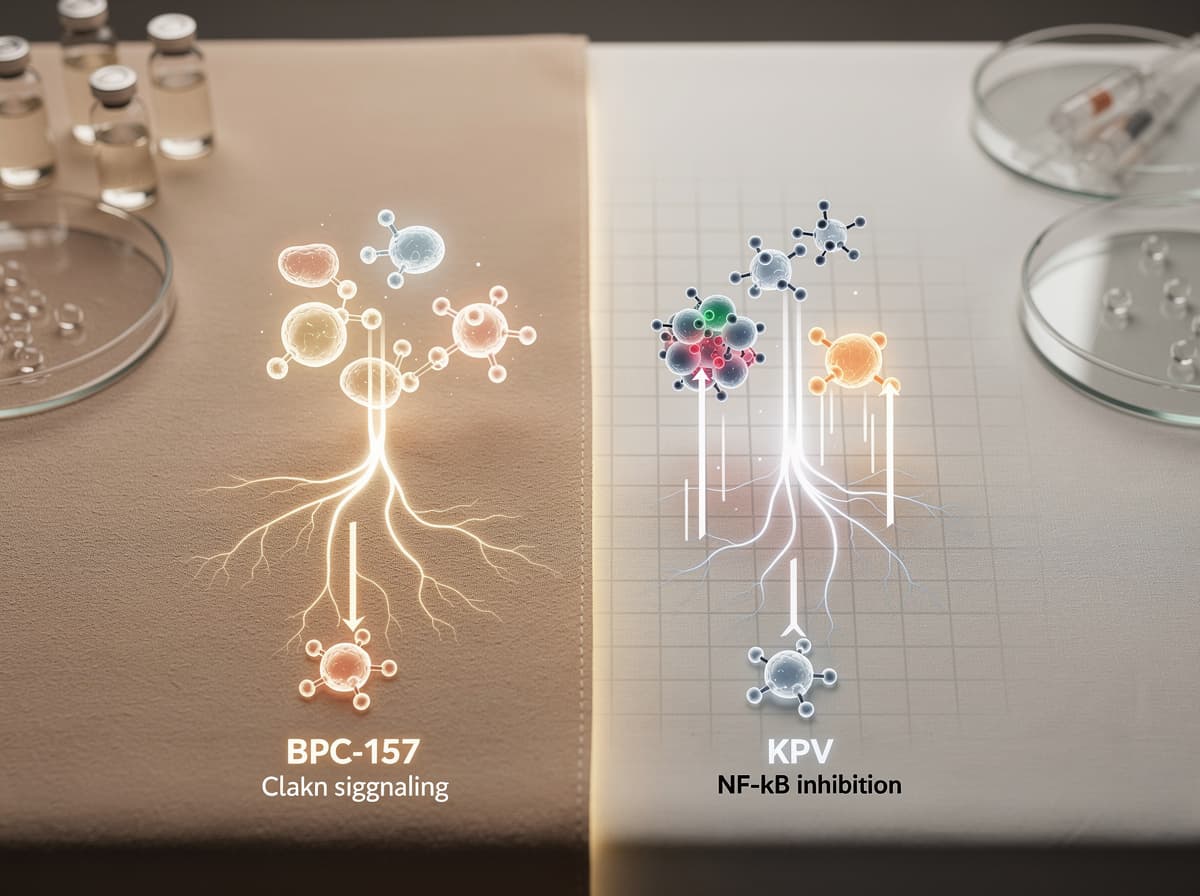
The mechanism is far more specific than BPC-157's. KPV inhibits the NF-κB and MAPK signalling cascades directly inside cells. Research has shown that KPV reduces the two most important intracellular signaling pathways in the pathogenesis of IBDs: the NF-κB and MAPK cascade pathways as well as the subsequent synthesis of proinflammatory cytokines . The result is reduced TNF-α, IL-1β, IL-6, IL-12, and IFN-γ output without the broad immunosuppression seen with corticosteroids.
What makes KPV unusually well-suited to gut work is its delivery route. In Caco2-BBE cells, hPepT1 has a high affinity for KPV with a Km around 160 μM that allows low doses of KPV to be efficiently targeted to the intracellular compartment; this Km is among the lowest reported for hPepT1, far below Gly-Sar which has a Km of at least 1 mM . PepT1 is upregulated in inflamed colonic tissue, so oral KPV preferentially accumulates where it is needed most. The transporter dependence is not theoretical: in PepT1-knockout mice, KPV's anti-inflammatory effect in the colitis model is abolished.
Dosing: BPC-157 vs KPV#
Both peptides have research-published dose ranges, not approved clinical doses. Every number below is a research protocol range, not a prescription.
For BPC-157, oral protocols in the research literature typically range from 250 to 500 mcg, taken once or twice daily. The animal data spans a wide range: in rat colitis studies, BPC 157 was applied at 10 μg/kg or 10 ng/kg intraperitoneally once daily, or 0.16 μg/ml in drinking water . Human-equivalent extrapolation from these rodent doses lands roughly at the 250-500 mcg/day band that has been published in protocol reviews. Timing is flexible because of the gastric-juice stability; food does not appear to matter.
For KPV, the research-published oral range is 200 to 500 mcg once daily, with some protocols extending to 1 mg. The mouse evidence anchored on a different unit: Dalmasso et al. demonstrated that oral KPV at 100 μM in drinking water reduced DSS-induced colitis severity by roughly 50% as measured by myeloperoxidase activity in mice . Timing matters more for KPV than for BPC-157: research protocols suggest dosing on an empty stomach so dietary peptides do not compete for PepT1 binding sites.
Evidence: what the studies actually show#
There is no head-to-head trial of BPC-157 versus KPV. The comparison has to be done across separate studies on separate models, and the asymmetry matters.
BPC-157 has the deepest animal evidence base of any gut-targeted peptide. The 2007 paper in the Journal of Pharmacological Sciences documented healing of colocutaneous fistulas at doses where sulphasalazine was only moderately effective and corticosteroids were actively harmful. Sulphasalazine was only moderately effective, and corticosteroid even had an aggravating effect in the same model. The animal data spans more than 30 years across colitis models, fistula healing, anastomotic repair, and barrier function. The human data is the gap: BPC-157 entered Phase II trials for ulcerative colitis under the designation PL 14736 and the trial completed, but results were never published in a peer-reviewed journal . Preliminary evidence is therefore strong in rodents and unverified in humans.
KPV has narrower but cleaner mechanistic evidence. The pivotal study is Dalmasso et al. 2008 in Gastroenterology: oral administration of KPV reduces the incidence of DSS- and TNBS-induced colitis indicated by a decrease in pro-inflammatory cytokine expression, and the study indicates KPV is transported into cells by PepT1 and might be a new therapeutic agent for IBD . Follow-up work using PepT1 gene silencing confirmed the transporter is necessary, not just facilitatory. No human IBD trial exists.
The evidence asymmetry is real: BPC-157 has breadth across tissue types but no published human results; KPV has narrow gut-specific mechanism with a confirmed transport pathway but no human trial at all.
Side effects and contraindication profile#
Both peptides have unusually clean safety profiles in the published animal literature, which is part of why they keep appearing in research protocols.
BPC-157's toxicology is summarised in nearly every Sikiric paper with a single phrase: LD1 not achieved. No toxic effect, limit test negative, LD1 not achieved, no side effect in trials has been the consistent finding across more than 30 years of rodent work. The PL 14736 Phase II trial reported no safety signal serious enough to halt the program. The realistic side-effect picture in protocol use is mild: occasional injection-site reactions when used subcutaneously, transient mild GI sensitivity orally, no documented liver or kidney signal.
KPV is similarly mild. Across the published animal studies, the adverse event spectrum is limited to injection-site redness, occasional mild nausea on high oral doses, and minor topical irritation. No deaths, organ toxicity, or dose-limiting adverse events have been documented in peer-reviewed literature at doses up to 10 mg/kg in rodent models, roughly 50 to 100 times the typical human-equivalent research dose . Because KPV does not broadly suppress immune function, it does not carry the infection-risk profile of biologics or corticosteroids.
Where they diverge: BPC-157 is on the WADA Prohibited List under category S0 since January 2022, so competitive athletes need to know that. KPV is not currently on the WADA list. The melanocortin lineage of KPV warrants one specific caution: active melanoma is a theoretical concern because of the parent hormone's role in melanocyte signalling, even though KPV itself is associated with the anti-inflammatory not pigmentary fragment.
Both substances were placed on the FDA's Category 2 bulk substances list in September 2023. The FDA added AOD 9604, BPC-157, Cathelicidin LL-37, CJC-1295, GHK-Cu for injectable routes, Ipamorelin Acetate, Kisspeptin-10, KPV, Melanotan II, Selank, Semax, Thymosin Alpha-1, and Thymosin Beta-4 fragment to Category 2 because FDA identified significant safety risks with these substances . This is a compounding-pharmacy restriction, not a possession ban; see Klarovel disclosures for how this shapes the protocol layer.
When to choose BPC-157#
BPC-157 is the better starting point when the clinical picture involves tissue damage that needs to be rebuilt, not just inflammation that needs to be quieted.
- Post-surgical gut healing, particularly anastomosis recovery, where the goal is structural repair and angiogenic support.
- Mixed musculoskeletal and gut presentations: a runner with both tendinopathy and reflux gets two effects from one peptide, since BPC-157 acts systemically.
- Suspected leaky-gut / barrier-permeability problems where mucosal integrity is the issue, not transcription-factor overactivation.
- Anyone who needs route flexibility: oral, subcutaneous, or intramuscular all have research-published precedent.
When to choose KPV#
KPV is the better starting point when the clinical picture is dominated by active inflammatory cytokine output in the gut or skin.
- Active mild-to-moderate colitis-pattern symptoms where NF-κB-driven cytokines (TNF-α, IL-6, IL-1β) are the suspected driver. PepT1 expression is upregulated in inflamed colonic tissue from both DSS-treated mice and human IBD patients, suggesting preferential KPV absorption at sites of inflammation .
- Inflammatory skin conditions (psoriasis-pattern, atopic dermatitis-pattern) where topical or systemic α-MSH-fragment immunomodulation is the mechanistic match.
- Patients who cannot tolerate the broader systemic effects of BPC-157 and want a narrower target.
- Anyone wanting the cleanest oral pharmacokinetics: the PepT1 affinity makes low-dose oral KPV genuinely targeted, not just hopeful.
Can you stack them?#
Yes, and the mechanism makes the pairing sensible. The two peptides hit complementary receptors and complementary biology: KPV silences the cytokine cascade upstream (NF-κB, MAPK), while BPC-157 rebuilds the damaged tissue downstream (angiogenesis, growth-factor signalling, collateral vessel recruitment). Their effects are supra-additive in concept because neither one fully covers what the other does.
There is no published trial of the BPC-157 plus KPV combination in humans, so any stacking remains in the realm of protocol convention rather than evidence. The practical configuration researchers use: oral KPV in the morning on an empty stomach to drive the PepT1-mediated colonic delivery, BPC-157 at a separate window (often evening) to avoid any peptidase or transporter competition. Both peptides are oral-stable, which removes the injection-burden argument against combining.
The honest caveat: stacking doubles the regulatory exposure and the cost without doubling the evidence base. For a first cycle, picking one based on the dominant clinical feature usually beats running both.
Verdict#
For most active gut-inflammation pictures where the dominant feature is cytokine overactivation (the colitis-pattern symptom cluster), KPV is the better starting point. Its mechanism is precise, its delivery route is genuinely targeted via PepT1, and its safety profile is cleaner because it does not broadly perturb other systems.
For most tissue-repair pictures where the dominant feature is structural damage that needs to heal (post-surgical, anastomotic, fistula, mixed gut-plus-musculoskeletal), BPC-157 is the better starting point. The breadth of the cytoprotective evidence is unmatched, and the gastric-juice stability removes most of the absorption uncertainty that plagues oral peptides.
Both are valid. The deciding question is not "which is stronger?" but "is the problem inflammation, or is it damage?" The Klarovel questionnaire plus a basic inflammatory panel (CRP, calprotectin if gut-targeted) usually resolves which side of that line a given case sits on.
Decide based on biology, not marketing#
The internet talks about BPC-157 and KPV as if they were competitors. They are not. They sit on different rungs of the inflammation-and-repair ladder, and a sober reading of the literature points to specific use cases for each. The mistake is picking one because it has louder marketing; the better move is picking one because the mechanism matches the problem.
The Klarovel peptide calculator handles the dose arithmetic once the choice is made, and the questionnaire walks through the symptom pattern that usually decides BPC-157 versus KPV in the first place. Start there, not with the order form. Then, if it makes sense to begin, register and get the protocol layer wired up properly.
Frequently asked questions
Keep reading
P21 vs Semax: which nootropic peptide wins in 2026?
P21 vs Semax head-to-head on mechanism, dosing, and evidence. One is a CNTF-derived neurogenic peptide, the other a Russian-approved BDNF booster.

Hexarelin vs MK-677: Ghrelin Mimetics Head-to-Head (2026)
Hexarelin's acute GH spike versus MK-677's oral 24-hour IGF-1 elevation. Which ghrelin-receptor agonist actually fits your research goal, and where each fails.

Epitalon vs NAD+: Which Longevity Path Fits You (2026)
Epitalon activates telomerase on short cycles; NAD+ precursors refill a daily metabolic cofactor. Head-to-head on evidence, dosing, and how to choose.