Nootropic-curious readers keep landing on the same fork in the road: P21, a small CNTF-derived peptide with strong rodent data on neurogenesis, or Semax, a Russian-registered ACTH fragment with two decades of intranasal use in stroke rehabilitation. They target different biology, sit at different regulatory maturities, and reward very different research goals. This comparison lays out the mechanism, the numbers, and a clear decision rule.
Key takeaways#
- P21 is a CNTF-derived neurogenic peptide with adamantane modification; Semax is an ACTH(4-7) analogue that upregulates BDNF within minutes of intranasal dosing.
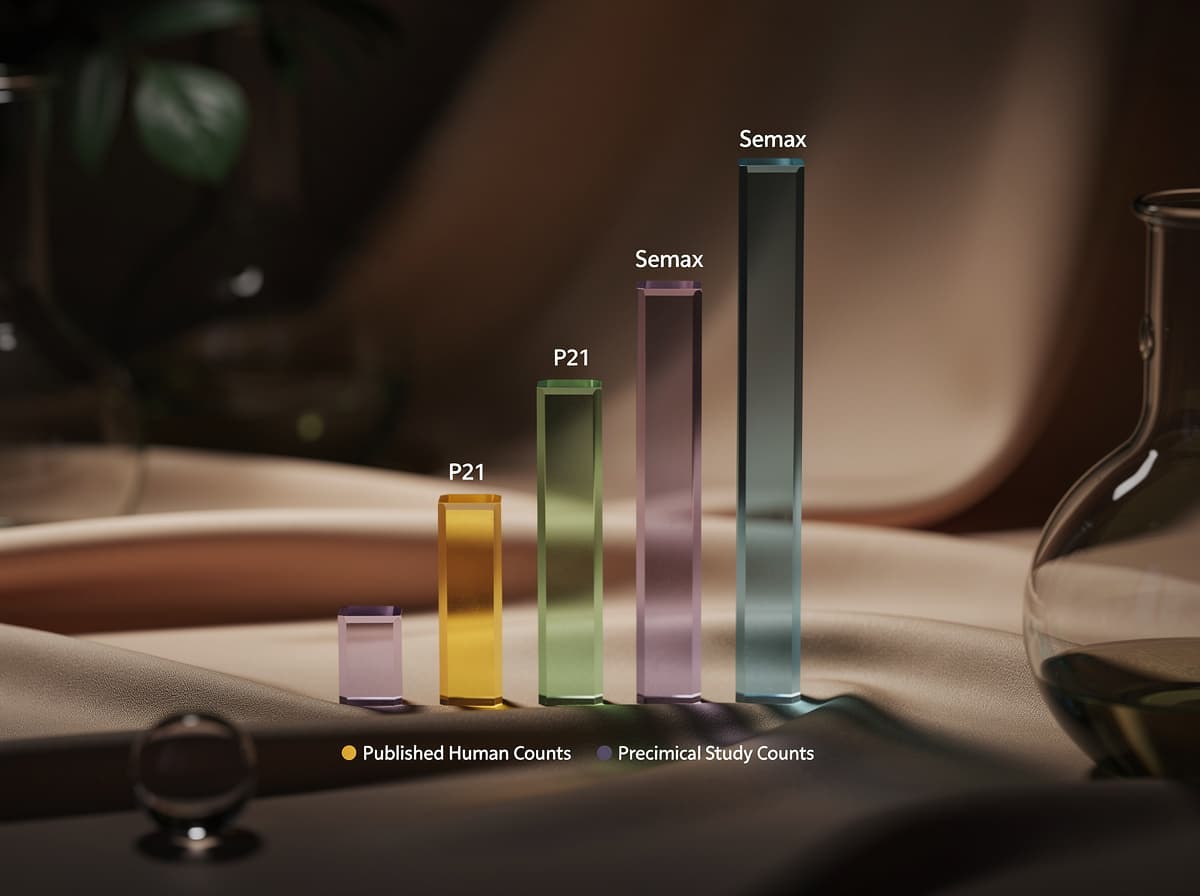
- Semax has human data (small trials, mostly Russian); P21 evidence is entirely preclinical and concentrated in one lab group.
- For hippocampal neurogenesis and tau-pathway research, P21 has the stronger mechanistic story; for acute neuroprotection and same-day cognitive effects, Semax has the stronger clinical footprint.
- Neither peptide has FDA or EMA approval. Semax is registered only in Russia; P21 has no regulatory approval anywhere.
- Stacking is theoretically complementary (BDNF upregulation on both sides plus neurogenesis on P21), but no head-to-head or combination human trial exists.
How P21 works#
P21 (also written P021) is a small synthetic peptide reverse-engineered from the active region of ciliary neurotrophic factor. Researchers reduced CNTF's neurogenic signal down to a short tetrapeptide core and added an adamantane group at the C-terminus for lipophilicity and protease resistance. Li and colleagues (2010) showed that the CNTF-derived peptidergic compound, P21, incorporating a γ-aminoadamantane-1-carboxylic acid at its C-terminus, is neurogenic and neuroplastic and enhances cognition in normal adult mice .
Mechanistically, P21 does not simply bind CNTF receptors. It appears to act upstream by inhibiting leukemia inhibitory factor (LIF) signalling, which in turn releases a brake on hippocampal neurogenesis and drives BDNF expression. That BDNF surge activates the TrkB-PI3K-Akt cascade, phosphorylates GSK-3β at serine 9, and reduces tau hyperphosphorylation downstream. In the 3xTg-AD mouse model, chronic oral P021 produced a significant reduction in abnormal hyperphosphorylation and accumulation of tau at known major AD neurofibrillary pathology associated sites, a significant decrease in soluble Aβ levels, and this disease modifying effect was probably via increased brain derived neurotrophic factor (BDNF) expression mediated decrease in glycogen synthase kinase-3-β (GSK3β) activity . Route in the published literature is chronic oral dosing; the peptide's adamantane group is what makes oral bioavailability plausible.
How Semax works#
Semax is a synthetic heptapeptide built from the ACTH(4-7) fragment with a Pro-Gly-Pro C-terminal tail that resists enzymatic breakdown. It has been used clinically in Russia since the 1990s and is delivered intranasally, which routes the peptide directly toward the central nervous system.
The dominant mechanism is rapid BDNF upregulation. Research has shown that Semax raises BDNF mRNA and protein in the hippocampus and basal forebrain within hours of a single dose, with parallel modulation of serotonergic and dopaminergic signalling. Beyond the trophic axis, transcriptional analysis in rat focal ischemia reported that Semax influenced the expression of genes that promote the formation and functioning of the vascular system, and the immunomodulating effect of the peptide and its impact on the vascular system during ischemia are likely to be the key mechanisms underlying the neuroprotective effects of the peptide . The ACTH(4-7) backbone also touches melanocortin receptor pathways and the enkephalin system, which is associated with Semax's mild anxiolytic and stress-buffering profile in the published literature.
Dosing: P21 vs Semax#
Dose ranges below reflect published research protocols. They are not use-guidance and both compounds sit outside FDA and EMA approval.
P21. Research doses are extrapolated from rodent oral dosing (typically 20-60 nmol/day in the Iqbal lab protocols) and are not standardised in humans. No published human clinical trial exists that would validate a human research dose. Human research-published doses for P21 are limited and not standardised; any figure encountered online should be treated as extrapolation, not validated protocol.
Semax. Research protocols vary sharply by endpoint:
- Cognitive-research protocols in the published Russian literature use 200-600 mcg/day intranasally via a 0.1% solution, split across the morning.
- The Lebedeva 2018 fMRI study used a single total intranasal dose of 1% Semax in healthy volunteers, with resting state fMRI carried out 3 times: directly before and 5 and 20 min after intranasal 1% Semax (14 subjects) or placebo (10 subjects), studying the topography of the resting state default mode network .
- Stroke-rehabilitation research uses 6,000 mcg/day for 10 days per course, with an interval between courses, as documented in the Gusev efficacy study.
Timing: Semax is typically dosed in the morning because of the alerting effect; P21 in preclinical work was delivered chronically with food.
Evidence: what the studies actually show#
There is no head-to-head trial of P21 versus Semax in humans or animals. The evidence bases sit at different maturity levels.
P21 evidence. Preclinical only. Preliminary evidence points to disease-modifying effects in Alzheimer's mouse models. Baazaoui and Iqbal reported that P021 rescued dendritic and synaptic deficits, boosted neurogenesis, and reversed cognitive impairment in transgenic AD mice . Across aged rats, a 3xTg-AD Alzheimer's model, and a Ts65Dn Down syndrome model, chronic P021 was reported to enhance neurogenesis, raise BDNF, reduce tau pathology, and improve maze learning. Preclinical data points converge in direction, but as one 2026 review notes, the literature is consistent in direction but largely single-lab and unreplicated in humans .
Semax evidence. Human data exists, though small and mostly Russian. In the Gusev BDNF study, 110 patients after ischemic stroke were examined, divided into early and late rehabilitation groups, each subdivided into semax+ and semax- subgroups, with a standard regimen of 2 courses of 6000 mcg/day for 10 days with 20 day interval . The conclusion: Early rehabilitation and administration of semax increase BDNF plasma level, speed functional recovery, and improve motor performance . In healthy volunteers, the Lebedeva default mode network study found measurable central nervous system signal changes after a single intranasal dose. Sample sizes remain small and Western replication is limited, which the Cognitive Vitality reviewers at the ADDF flag explicitly.
Side effects and contraindication profile#
Both compounds have relatively clean short-term safety signals in the published literature, but the data density is very different.
Semax. Reported side effects are mild in the Russian clinical record and include nasal irritation, transient headache, and occasional gastrointestinal symptoms. No addiction potential and no withdrawal syndrome have been reported in published protocols. Long-term safety, route-specific adverse events, drug interactions, and special-population risks remain insufficiently characterised in Western literature.
P21. No human safety data exists. Rodent studies have not reported major adverse effects at chronic oral doses, and no retractions or expressions of concern have been noted across the P21 literature, which distinguishes it from some other frontier nootropic peptides. But absence of reported harm in a small rodent literature is not a safety file. Contraindications, interactions, and immunogenicity risk are all open questions.
Where they overlap: both act on the BDNF axis, so theoretical caution is warranted in anyone with a history of tumours where BDNF signalling could be permissive. Where they diverge: Semax's melanocortin-adjacent activity introduces a different profile from P21's LIF-inhibition axis, and only Semax has the intranasal route that can occasionally provoke local nasal reactions.
When to choose P21#
- The research goal is hippocampal neurogenesis or tau-pathway modulation, and rodent-model data is acceptable as the evidence base.
- The reader wants an orally administered peptide with a defined chemical identity, rather than an intranasal delivery route.
- The context is long-horizon neurodegenerative-model work where the BDNF-TrkB-GSK3β cascade is the specific target of interest.
- The user is comfortable operating on preclinical evidence with no human trial validation.
When to choose Semax#
- The research goal is acute cognitive or attentional effect, where a single-dose signal within 20-40 minutes matters.
- The context is post-ischemic rehabilitation research, where Semax has the strongest human data of any nootropic peptide currently available.
- The reader wants at least some human trial data, even if small and Russian-sourced.
- The delivery route needs to be non-injectable and easy to titrate; intranasal 0.1% solutions make dose fractionation practical.
Can you stack them?#
Combining P21 and Semax is not standard practice, because no combination trial (human or animal) exists in the peer-reviewed record. Mechanistically, the stack is not obviously conflicted: Semax delivers a rapid, transient BDNF surge, and P21 drives a slower neurogenic and anti-tau signal via a partially overlapping downstream pathway. The paired effect could in principle be complementary, but that is speculation, not data. Anyone stacking is running an unvalidated protocol; the sensible path is to run one peptide at a time, log endpoints, and let a signal separate from noise before layering.
Verdict#
For most nootropic-curious research contexts in 2026, Semax is the better starting point. It has human data (however imperfect), a defined intranasal protocol, and a rapid, observable acute effect that lets the researcher tell whether they are getting a signal. P21 is the more scientifically interesting molecule, with a cleaner mechanism story and stronger disease-model data, but its complete absence of human trials makes it the wrong first move for anyone who wants to see a response in weeks rather than years. Choose P21 only if the specific interest is hippocampal neurogenesis or tau pathway research and preclinical evidence is acceptable.
Turn the comparison into a decision#
The peptide that is right for a given research question depends on what the reader's biology is actually asking for, not on which molecule has the better marketing. Klarovel's peptide calculator and intake questionnaire turn the P21-vs-Semax fork into a data-driven answer keyed to individual endpoints. Deeper reading on each compound: the P21 complete guide, the Semax complete guide, and the Klarovel disclosures page for supplier and regulatory framing.
Frequently asked questions
Keep reading

Hexarelin vs MK-677: Ghrelin Mimetics Head-to-Head (2026)
Hexarelin's acute GH spike versus MK-677's oral 24-hour IGF-1 elevation. Which ghrelin-receptor agonist actually fits your research goal, and where each fails.

Epitalon vs NAD+: Which Longevity Path Fits You (2026)
Epitalon activates telomerase on short cycles; NAD+ precursors refill a daily metabolic cofactor. Head-to-head on evidence, dosing, and how to choose.
BPC-157 vs Thymosin Alpha-1: Healing vs Immune Modulation (2026)
BPC-157 targets tissue repair and gut lining; thymosin alpha-1 modulates T-cell immunity. Head-to-head on mechanism, dosing, side effects, and stacking.