Most peptide content treats individual molecules as standalone tools. That framing hides the more useful truth: ipamorelin, CJC-1295, MK-677, and tesamorelin all act on the same regulatory circuit, and understanding that circuit predicts which compound fits which goal. This pillar walks through the GH peptide axis, the receptors involved, and how age changes the picture.
Key takeaways#
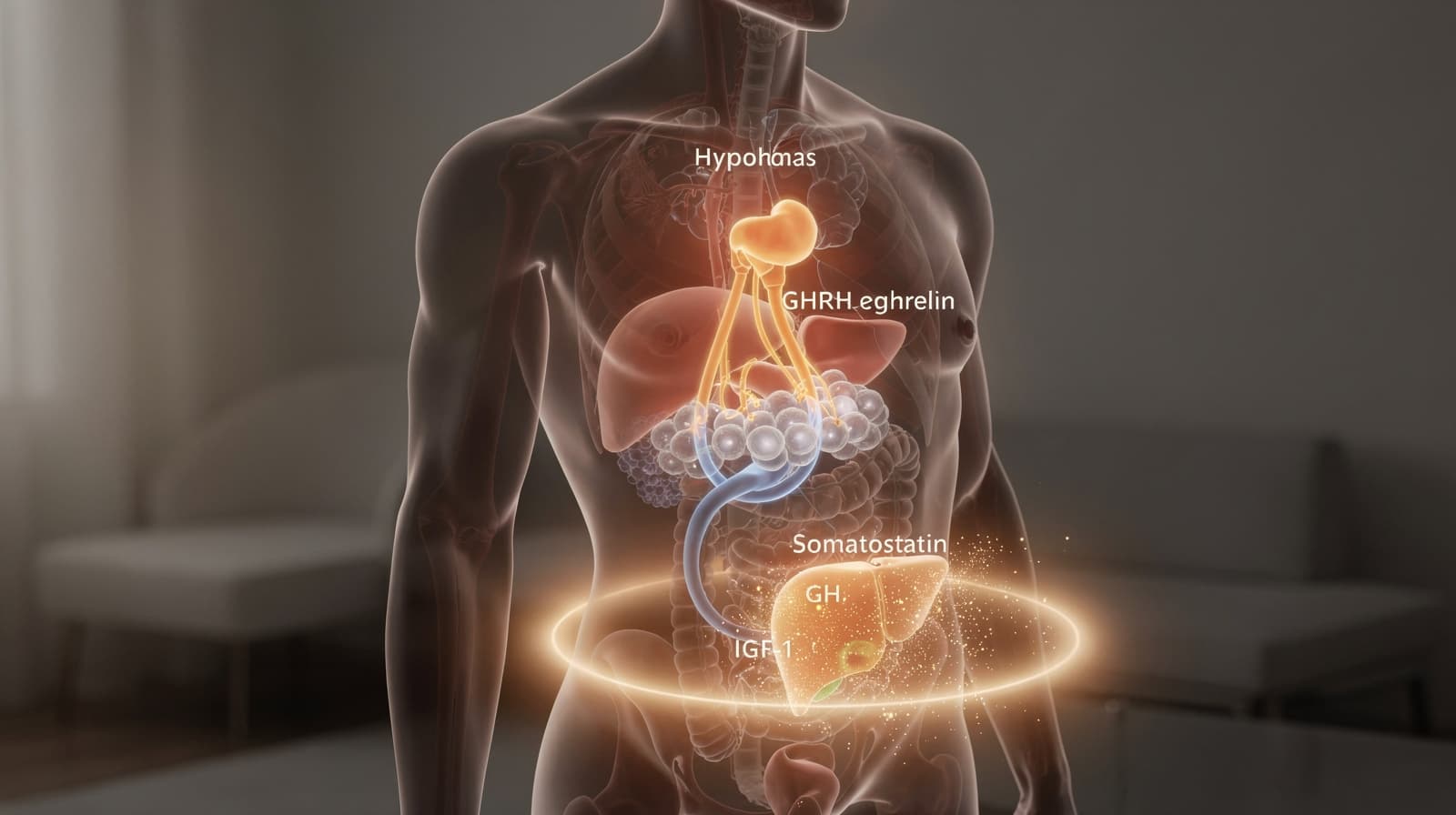
- The GH axis is governed by three inputs: hypothalamic GHRH (stimulatory), somatostatin (inhibitory), and stomach-derived ghrelin (stimulatory through a separate receptor).
- Pituitary somatotrophs release growth hormone in pulses; downstream hepatic IGF-1 closes the feedback loop by suppressing further GH output.
- Research suggests two receptor families are relevant for peptide protocols: the GHRH receptor (targeted by CJC-1295 and tesamorelin) and the GHSR-1a ghrelin receptor (targeted by ipamorelin and MK-677).
- Somatopause, the age-related decline in GH and IGF-1, has been shown to track with shifts in body composition and is associated with reduced lean mass.
- Pairing a GHRH analog with a ghrelin mimetic produces a supra-additive pulse, which is the mechanistic rationale behind common combination protocols.
The axis is a three-input control loop, not a single switch#
The classical description of growth hormone regulation, refined since the 1960s, has GHRH and somatostatin as opposing hypothalamic inputs. Pituitary synthesis and secretion of GH is stimulated by episodic hypothalamic secretion of GH releasing factor and inhibited by somatostatin, and Insulin-like Growth Factor I (IGF-I) inhibits GH secretion by a negative loop at both hypothalamic and pituitary levels.
That two-input model held until 1999, when the discovery of ghrelin added a third regulator from outside the brain. The gastric peptide ghrelin is also a potent GH secretagogue, which acts to boost hypothalamic GHRH secretion and synergize with its pituitary GH-stimulating effects. In other words, ghrelin hits a distinct receptor (GHSR-1a) and amplifies the GHRH signal both centrally and at the somatotroph.
The practical implication: any peptide that influences GH output has to act through one of these three control points. GHRH analogs push the accelerator. Ghrelin mimetics push a different accelerator. Nothing currently available in research-peptide form removes the somatostatin brake directly, which is why protocols time injections around endogenous somatostatin lows (typically before sleep or in the early morning fasted state).
GH release is pulsatile, and the pulse pattern matters more than the average#
Continuous GH exposure does not reproduce the physiology of healthy GH secretion. Studies have shown that GH secretion in man is pulsatile and this pattern is regulated by both GHRH and somatostatin, with bursts of GH secretion mediated by a reduction of tonic hypothalamic somatostatin secretion.
This is why long-acting recombinant GH and a well-designed peptide protocol produce different downstream signatures. A short GHRH pulse layered on top of an endogenous somatostatin trough preserves the pulse architecture; continuous receptor occupation does not. Research has shown the GH response to sustained GHRH infusion attenuates within hours, confirming that the somatostatin brake, not GHRH supply, dictates pulse timing.
For protocol design, three points follow:
- Timing relative to meals matters because nutrient intake suppresses GH and elevates somatostatin.
- Timing relative to sleep matters because the largest endogenous GH pulse occurs in early slow-wave sleep.
- Combining a GHRH analog with a ghrelin mimetic is associated with a larger pulse than either compound alone, because the two receptors converge on the same somatotroph through complementary action.
Two receptor families, two peptide categories#
Every peptide marketed as a "growth hormone secretagogue" falls into one of two mechanistic buckets, defined by the receptor it binds.
GHRH receptor agonists mimic endogenous GHRH at the pituitary GHRH receptor. Growth Hormone-Releasing Hormone (GHRH), secreted by neurons in the arcuate nucleus of this brain structure, stimulates HGH production in the anterior pituitary gland. CJC-1295 and tesamorelin are the two compounds most often discussed in this category. Tesamorelin is the only FDA-approved GHRH analog, studied primarily in HIV-associated lipodystrophy. Klarovel covers tesamorelin's mechanism and trial data in the tesamorelin guide.
Ghrelin receptor agonists (also called GHSR-1a agonists, growth hormone secretagogues, or "GHS") bind the receptor that endogenous ghrelin activates. Research has shown that ghrelin exerts a synergistic effect with GHRH in the induction of GH secretion ; this is the receptor that ipamorelin and MK-677 target. Ipamorelin is an injected, short-acting peptide; MK-677 (ibutamoren) is an orally bioavailable non-peptide ghrelin mimetic. The mechanistic comparison is laid out in the MK-677 guide and the ipamorelin overview.
The reason combination protocols exist is precisely because these are two different receptors with complementary downstream signaling. The paired CJC-1295 plus ipamorelin approach is covered in detail in Klarovel's CJC-1295 and ipamorelin protocol article.
Somatopause shifts the baseline that protocols try to address#
The biological reason interest in GH-axis peptides exists is that the axis attenuates with age. Research has shown that GH production and secretion, GH binding protein, and IGF-1 levels decline with aging, often referred to as the "somatopause", and these decrements provide the basis for speculation that these anabolic hormones are related to body composition, metabolic, and functional changes that occur with aging.
The numbers are starker than most people expect. After puberty, GH levels decrease exponentially, production is reported to decline by 14% per decade and may decline by up to 50% every seven years for adult men, with elderly men producing as little as 50 μg/day compared with pubertal boys who produce 1.0 to 1.5 mg/day. Studies have shown the resulting state is associated with increased adipose tissue and the broader cluster of changes that mirror clinical adult GH deficiency.
A second clinical review frames the mechanism plainly: age-related decline in GH levels is very well documented, consistent across different mammalian species and primarily due to reduced hypothalamic secretion of GHRH with consequent decline of GH biosynthesis and release by the anterior pituitary, which leads to a reduction in circulating levels of insulin-like growth factor 1 (IGF-1), the key mediator of GH action.
Two preliminary findings matter for protocol thinking. First, the decline is upstream: it starts with GHRH, not with somatotroph capacity, which is why GHRH analogs remain effective in older subjects. Second, the tesamorelin literature documents that the GHRH agonist restores normal GH pulsatility and amplitude, selectively reduces visceral fat, intima media thickness and triglycerides, and improves cognitive function in older persons. Preliminary evidence points toward restoring pulse architecture, not flooding the system with continuous GH.

Feedback loops and side-effect mechanisms come from the same diagram#
Reading the axis as a loop also explains why some compounds cause specific tolerability profiles. Three feedback nodes matter:
- IGF-1 negative feedback at the hypothalamus. Rising hepatic IGF-1 inhibits GHRH neurons and stimulates somatostatin. This is why chronic high-dose ghrelin agonism, especially with oral MK-677, can plateau over weeks: the elevated IGF-1 closes the loop and dampens further GH amplitude.
- Ghrelin's orexigenic action. The same receptor that drives GH release also drives hunger. Research has shown that ghrelin is an orexigenic hormone, released primarily by the gastric mucosa, although it is widely expressed in many different tissues, including the central nervous system and the pituitary. Increased appetite on MK-677 is not a side effect; it is on-target pharmacology.
- Insulin and glucose handling. GH is counter-regulatory to insulin. Studies have shown that during prolonged GH elevation, hepatic gluconeogenesis and free fatty acid mobilization rise, which can blunt insulin sensitivity. The peptide calculator integrates this when modelling pulse exposure over a cycle.
A separate point worth flagging: somatostatin inhibits GH secretion and regulates multiple processes by signaling through its receptors sst1 to sst5, and differential expression of these receptors may contribute to sex-specific GH patterns and fasting-induced GH rise. Translation: protocol responses differ by sex and feeding state, and a single dose recommendation across populations is rarely defensible.
How the four GH-axis peptides map onto this circuit#
Putting it together, the four peptides Klarovel covers in depth occupy distinct positions on the same diagram:
- Ipamorelin: short-acting selective GHSR-1a agonist. Produces a clean GH pulse without significant cortisol or prolactin elevation. Best for users who want pulsatile, time-bounded stimulation.
- CJC-1295 (with or without DAC): GHRH receptor agonist. Without DAC, behaves like a short GHRH pulse; with DAC, provides sustained GHRH receptor exposure. Often paired with ipamorelin to engage both receptors.
- MK-677 (ibutamoren): orally bioavailable, long-acting GHSR-1a agonist. Maintains elevated 24-hour GH and IGF-1 averages but loses pulse architecture and engages the orexigenic and water-retention effects of ghrelin signalling more visibly.
- Tesamorelin: stabilised GHRH analog with the clearest clinical evidence base, specifically for visceral adipose tissue reduction in HIV-associated lipodystrophy per its FDA labelling.
For a fuller framework on how to compare these candidates, see how Klarovel structures protocol curation, and run dose-window scenarios through the peptide calculator. Account holders can save protocol templates via register.
Read more on Klarovel#
- CJC-1295 + Ipamorelin: the GH stack mechanism explained: The CJC-1295 + Ipamorelin stack pairs a GHRH analogue with a GHRP for amplified GH pulses.
- Ipamorelin: the cleanest GHRP in the research catalogue: Ipamorelin is the most selective ghrelin mimetic in the GHRP class, with no meaningful cortisol or prolactin lift.
- Ipamorelin vs CJC-1295: GHRP vs GHRH Head-to-Head (2026): Ipamorelin vs CJC-1295 settled: one is a ghrelin-receptor pulse, the other a GHRH analog with a six-day half-life.
- Ipamorelin vs MK-677: Pulsatile or Sustained GH (2026): Injectable ipamorelin vs oral MK-677: pulsatile pulses versus 24-hour elevation.
- MK-677 (ibutamoren): the oral GH secretagogue explained: MK-677 (ibutamoren) is the only orally active growth hormone secretagogue.
- Peptides for Muscle Growth: What the 2026 Data Says: Trials report 1.1 to 1.3 kg lean mass gain on growth-hormone peptides over 6 to 12 months.
- Peptides vs HGH: Is This Just Expensive Growth Hormone?: Peptides vs HGH compared on mechanism, dosing, side effects, and US legal status.
- Tesamorelin (Egrifta): the FDA-approved GHRH analogue: Tesamorelin is a stabilised GHRH analogue with FDA approval for HIV-associated lipodystrophy.
The axis view changes which questions are worth asking#
Instead of asking "which peptide is best", a working knowledge of the GH peptide axis reframes the question: which receptor, which pulse pattern, which feedback regime fits the goal. That framing is what Klarovel's protocol curation is built around. Start with the peptide calculator to model a candidate protocol, review the regulatory framing in our disclosures, and register to save your work and follow the cluster updates as new evidence lands.
Frequently asked questions
Keep reading

GLP-1 Weight Loss Plateau: Why It Happens and What Works
GLP-1 plateaus arrive near week 60 in most trials. Here is the physiology, what the STEP and SURMOUNT data actually show, and how to respond intelligently.

Peptides for Brain Fog: What the Long-COVID Research Shows
An evidence-based look at peptides studied for post-viral brain fog: mechanisms, the cognitive peptide candidates, and what the long-COVID data actually says.

Peptides for ADHD: What Semax Research Actually Shows
Best peptide for ADHD focus? An honest look at Semax, Selank, and BDNF mechanisms, plus what the preclinical and pilot data actually support in 2026.