Few molecules in male hormone research generate more confusion than human chorionic gonadotropin. It sits at the intersection of fertility clinics, testosterone replacement protocols, and bodybuilding folklore, and the signal-to-noise ratio reflects that. This guide walks through what the peer-reviewed literature actually says about hCG in men: what it does at the receptor level, why clinicians add it to testosterone replacement, what the dose-response data look like, and where the real safety questions live.
Key takeaways#
- hCG binds the same testicular LH receptor that pituitary luteinizing hormone uses, which is why it can stimulate Leydig cells to make intratesticular testosterone even when the brain has stopped signalling.
- Exogenous testosterone suppresses intratesticular testosterone, and up to 40% of men on testosterone replacement develop azoospermia; hCG is the primary tool used to counter this.
- Research suggests 500 IU every other day raises intratesticular testosterone roughly 26% above baseline, while 250 IU every other day falls about 7% below baseline.
- A randomised comparison found 5,000 IU of hCG twice weekly produced testosterone responses similar to 50 mg clomiphene in hypogonadal men.
- The most consistent dose-dependent side effect is elevated estradiol from aromatisation, which can drive gynecomastia at higher doses.
How hCG actually works in the testis#
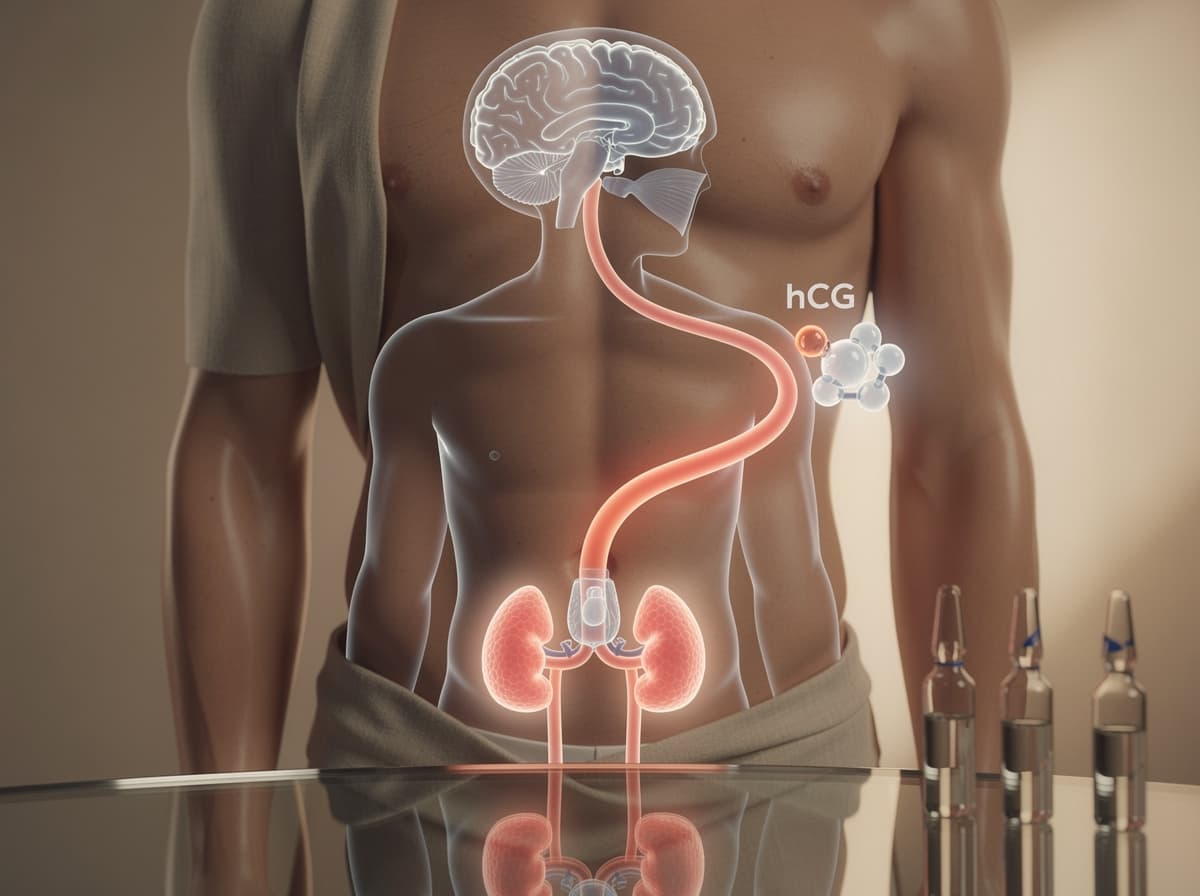
hCG is a glycoprotein hormone built from an alpha and a beta subunit. hCG is a hormone comprising of an α and a β-subunit, and hCG and LH share an identical α-subunit. The shared structure is the entire pharmacological story: because hCG looks enough like luteinizing hormone at the receptor, it binds the LH receptor on Leydig cells and triggers the same steroidogenic cascade. Luteinizing hormone acts on the Leydig cells, stimulating steroid production.
That receptor crosstalk matters because spermatogenesis is not driven by serum testosterone. It is driven by intratesticular testosterone (ITT), a local concentration that runs roughly ten times higher than what shows up in a blood draw. High intratesticular testosterone levels, usually higher than serum testosterone levels, seem to be necessary for healthy spermatogenesis in men. When a man injects exogenous testosterone, his pituitary stops sending LH, the Leydig cells go quiet, and ITT collapses even though serum testosterone looks fine on labs. Exogenous testosterone suppresses intratesticular testosterone production, which is an absolute prerequisite for normal spermatogenesis, and cessation of exogenous testosterone should be recommended for men desiring to maintain their fertility.
hCG is how clinicians keep the Leydig cells working when the upstream signal has been silenced.
Why TRT alone breaks fertility and what hCG does about it#
The fertility cost of testosterone replacement is not theoretical. Testosterone replacement therapy results in decreased serum gonadotropins and intratesticular testosterone, and impairs spermatogenesis, leading to azoospermia in 40% of patients. The American Urological Association now recommends hCG specifically for testosterone-deficient men who want to keep the option of biological children open. The American Urological Association guidelines recommend hCG for T-deficient men with fertility concerns, as it prevents azoospermia seen in up to 60% of men on exogenous T.
The mechanism for this rescue is straightforward. hCG acts as an LH analogue, binding the same receptors and stimulating local testosterone production inside the testis. hCG is similar in structure to luteinising hormone, which is a hormone produced by the pituitary gland that stimulates the production of testosterone in the testes, and hCG acts as a LH analogue, binding to the same receptors in the testes and stimulating the production of testosterone.
A randomised controlled trial in 56 men on testosterone-induced gonadotropin suppression compared 250 IU hCG every other day against placebo on top of TRT. After 24 weeks, the hCG group had significantly higher intratesticular testosterone than placebo. A separate study has shown that low-dose hCG concurrent with testosterone replacement appears to maintain semen parameters in hypogonadal men, and the authors concluded the combination may preserve fertility in men who want it while on TRT.
For men who already arrived at the fertility clinic with azoospermia from prior testosterone use, the rescue pathway is more aggressive. One retrospective series used 3,000 IU of hCG subcutaneously every other day combined with clomiphene, tamoxifen, anastrozole, or recombinant FSH depending on the case.
What the dose-response data actually show#
Most dosing arguments online happen because people skip the intratesticular testosterone data. The numbers are unusually clean. Research on ITT levels showed that 250 IU every other day produced ITT levels 7% below baseline, while 500 IU resulted in ITT 26% above baseline. The same Baylor work demonstrated that 500 IU every other day maintained normal sperm parameters in men on testosterone, with several couples achieving pregnancy during the study window.
Translated into practical research protocols:
-
Testicular size preservation only (no fertility goal): preclinical data points and clinical experience suggest 1,500 IU of HCG given weekly is enough to maintain pre-TRT levels of intratesticular testosterone.
-
Active fertility protocol on TRT: 500 IU every other day is the most consistently cited dose in published series.
-
Hypogonadism monotherapy (no TRT): the published monotherapy series used varying doses of HCG (range: 1000–3000 international units, twice a week) with a mean dose of roughly 1,529 IU.
-
Post-TRT axis restart: higher pulsed doses, typically dropped before transitioning to a SERM.
The 5,000 IU twice-weekly comparison against clomiphene is instructive because it sets a ceiling. Patients were randomly assigned to one of three groups: 50 mg of CC, 5000 IU of HCG two times per week, or a combination, for 3 months, and serum testosterone levels were upregulated from 66 ng/dL to 149 ng/dL, a 223% increase, with no major difference between the groups. More hCG did not mean more testosterone above a certain threshold; it just meant more aromatisation.
hCG as monotherapy: the "normal testosterone but symptomatic" question#
One of the more interesting recent lines of research is hCG used alone in men who feel hypogonadal but whose serum testosterone is technically above the 300 ng/dL TRT threshold. A 2022 series enrolled 31 men, aged 25 to 79, experiencing hypogonadal symptoms with average testosterone levels above 300 ng/dL, who received varying doses of HCG, range 1000 to 3000 IU twice a week.
The symptom data were striking. When evaluated for improvement of ED and low libido, 86% (19/22) and 80% (20/25) of patients reported improvement of each symptom, respectively. Equally important was what did not change: there was no significant change in serum T, FSH, PSA, HCT, estradiol, A1c or LH across the follow-up window. No thromboembolic events or hCG side effects, including headache, gynecomastia, and gastrointestinal issues, were observed.
This is a small, single-centre study and should not be read as a green light. It is, however, preliminary evidence that the LH signal itself, independent of the serum testosterone number, may matter for some men.
Side effects, real and overstated#
The side effect profile of hCG is dominated by one mechanism: aromatisation. Stimulating the Leydig cells produces testosterone, and a fraction of that testosterone is converted to estradiol by aromatase. HCG mimics LH to stimulate testicular testosterone production; the resulting increase in aromatisation raises oestradiol levels.
That single pathway explains most of what shows up in the published adverse event lists:
-
Gynecomastia. This is the side effect most consistently associated with hCG in men, and it is dose-dependent. Gynaecomastia is a recognised adverse reaction to HCG, caused by elevated oestradiol stimulating oestrogen receptors in male breast tissue, leading to glandular proliferation.
-
Mood and emotional lability. Reported in some series, attributed to shifting estradiol-to-testosterone ratios.
-
Injection site reactions. Pain, redness, and local swelling are the most common patient-reported issues.
-
Rare thromboembolic events. Studies have shown a small signal in patients with underlying clotting disorders, which is why screening matters before any protocol begins.
A second category is worth flagging because the marketing world will not. hCG is contraindicated in men with active prostate cancer, since the testosterone rise it generates is androgen-receptor active. Anyone with a PSA trend that needs investigation should resolve that before considering an hCG protocol.

Where hCG sits versus clomiphene and enclomiphene#
The most common alternative to hCG in hypogonadism is a selective estrogen receptor modulator like clomiphene citrate or its purified isomer enclomiphene. Mechanistically these sit one step upstream of hCG: instead of mimicking LH at the testis, SERMs block estrogen feedback at the hypothalamus and pituitary, so the brain releases more of its own LH and FSH.
The trade-offs are well documented. Clomiphene is oral, cheaper, and easier to obtain in most jurisdictions. Off-label use of SERMs, such as clomiphene citrate, are effective for maintaining testosterone production long-term and offer the convenience of representing a safe, oral therapy. hCG works regardless of whether the pituitary is functional, which makes it the only option in true secondary hypogonadism where the upstream signal is genuinely missing. HCG can be very effective, with no side effects on fertility, and safe for patients with secondary hypogonadism, however, HCG can be expensive or not easily available depending on the country.
A clean comparison: research-grade hCG is available from specialised suppliers, and Klarovel does not stock or sell peptides. The protocol layer, lab interpretation, and supplier evaluation are what we curate. For dose math, the peptide calculator converts the IU labelling on hCG vials to volume per click, which is where most research protocol errors happen.
How Klarovel approaches hCG protocols#
hCG sits in an unusual category. It has decades of peer-reviewed data, a clear mechanism, and a defined place in mainstream urology guidelines, yet most of the consumer-facing content about it is either bodybuilding lore or weight-loss marketing. The protocol design questions, dose, frequency, monitoring cadence, when to add a SERM or aromatase inhibitor, are exactly where most men get the worst advice.
Klarovel does not sell peptides. Research-grade hCG is available from specialised suppliers; we curate the protocol layer, the lab interpretation framework, and the comparison logic between hCG, SERMs, and TRT. Read how it works for the full model, or skim our disclosures for the boring legal version.
The bottom line on hCG for men#
hCG is one of the better-characterised molecules in male hormone research. It does one thing, it does it through one receptor, and the dose-response curve is unusually well documented. The questions worth spending time on are not whether it works, but at what dose, for which goal, and with what monitoring. Build that protocol on primary data, not on the loudest voice in a forum.
Create a free Klarovel account to access the full protocol library, lab interpretation tools, and the peptide calculator that does the IU-to-volume math correctly the first time.
Frequently asked questions
Keep reading
Hexarelin Peptide: The Forgotten GHRP and Why It Faded
Hexarelin was once the most potent GHRP known. Research suggests tachyphylaxis and CD36 side effects explain why the peptide world moved on.

Tesofensine: The Fourth-Class Weight Loss Peptide Guide
Tesofensine is a triple monoamine reuptake inhibitor that produced 10.6% weight loss in Phase 2. Mechanism, doses, safety, and GLP-1 comparison.

Peptides for Bodybuilding: What the GH-Axis Research Shows
A clinical look at GH-axis peptides used in physique work: what the human trials on MK-677, CJC-1295 and ipamorelin actually document, plus WADA rules.