
Both peptides are pitched in wellness clinics as gentle ways to nudge the growth hormone axis. They are not interchangeable. Ipamorelin and sermorelin act on two different receptors, produce two different pulse shapes, and suit two different reader profiles. This piece breaks the comparison down to the level where you can actually pick one.
Key takeaways#
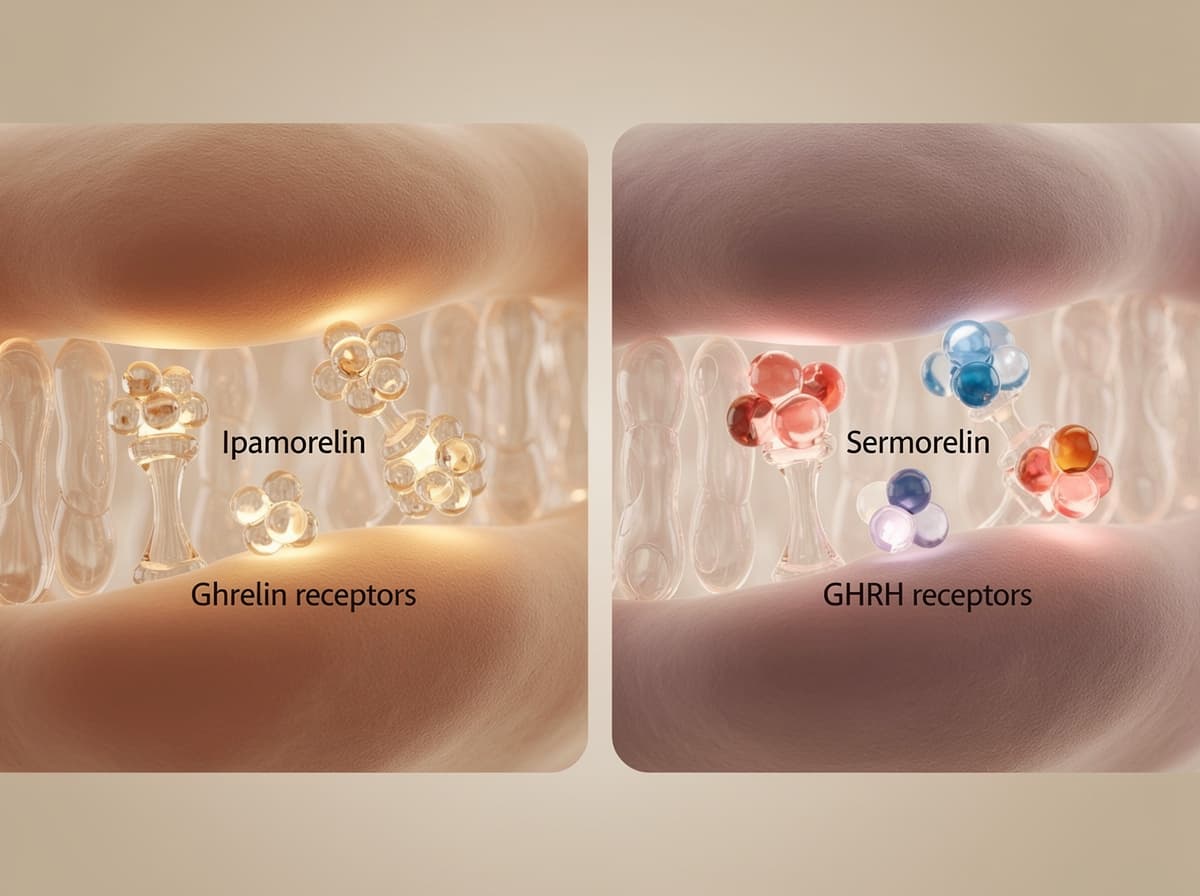
- Ipamorelin is a pentapeptide ghrelin-receptor agonist; sermorelin is a 29-amino-acid GHRH analog. They hit complementary receptors on the same somatotroph cell.
- Sermorelin has a plasma half-life of roughly 11-12 minutes; ipamorelin sits closer to 2 hours. Both still produce a discrete GH pulse rather than continuous elevation.
- Sermorelin is the only one of the two with formal FDA approval history (Geref, 1990s, for paediatric GH deficiency and as a diagnostic test).
- Side-effect profiles overlap on injection-site reactions and mild flushing; ipamorelin is more selective and leaves cortisol, prolactin, and ACTH essentially untouched.
- For most adult readers asking "which one to start with," sermorelin has the deeper human safety record. Ipamorelin has the cleaner endocrine fingerprint and the more flexible daytime dosing.
How ipamorelin works#
Ipamorelin is a synthetic pentapeptide with the sequence Aib-His-D-2-Nal-D-Phe-Lys-NH2, derived from the GHRP-1 scaffold. It binds the growth hormone secretagogue receptor (GHS-R1a), the same G-protein-coupled receptor that endogenous ghrelin uses to trigger GH release from anterior pituitary somatotrophs. In vitro, ipamorelin releases GH from primary rat pituitary cells with potency and efficacy similar to GHRP-6, and pharmacological profiling demonstrates that it stimulates GH release via a GHRP-like receptor rather than the GHRH receptor , as described in the original Raun et al. development paper.
The selling point that has kept ipamorelin in clinical conversation for 25 years is its receptor selectivity. Ipamorelin significantly and selectively increases plasma GH levels without any change in prolactin, follicle-stimulating hormone, luteinizing hormone, thyroid-stimulating hormone, adrenocorticotropic hormone, or cortisol levels in swines, and induces GH release with a peak at roughly 0.67 hours after administration followed by a rapid decline in healthy subjects . That selectivity is what differentiates it from the older GHRPs like GHRP-6, which carried more off-target endocrine noise. Plasma half-life after subcutaneous injection sits around two hours, which is why research-published protocols typically place doses near bedtime to stack the pulse onto the deep-sleep GH surge.
How sermorelin works#
Sermorelin is a 29-amino-acid synthetic analog corresponding to the first 29 residues of human growth hormone-releasing hormone (GHRH 1-29). Despite being a fragment of the natural 44-amino-acid molecule, the 1-29 region retains the full biological activity of GHRH. It binds the GHRH receptor on pituitary somatotrophs, which raises intracellular cAMP and triggers a physiologic GH pulse.
The defining pharmacokinetic feature is speed of clearance. After subcutaneous administration of 2 mg sermorelin, peak concentrations are reached in 5-20 minutes, sermorelin is rapidly cleared from the circulation with adult clearance values between 2.4 and 2.8 L/min, and the half-life is short, 11-12 minutes after either intravenous or subcutaneous administration , according to the Ishida et al. review in JCSM Rapid Communications. That blade-fast clearance is not a bug. It is the design intent: a brief stimulus that lets the pituitary fire one pulse and then return to baseline, preserving the somatostatin feedback loop that keeps GH within physiologic range.
Research has shown that the biological consequence of that 12-minute peptide window is a 2-4 hour downstream GH pulse, because receptor binding kinetics, not plasma residence time, determine the effect. This is the practical reason sermorelin can be dosed once nightly without continuous infusion.
Dosing: ipamorelin vs sermorelin#
Ipamorelin doses in the research literature and community-protocol space cluster in the 100-300 mcg per injection range. Studies have shown linear dose-response in early human pharmacokinetic work, and the curve flattens above roughly 300 mcg per shot, so escalating past that ceiling adds side-effect risk without proportional GH gain. Research protocols typically run a single subcutaneous shot at bedtime on an empty stomach, with some protocols splitting into two or three smaller daily doses. Cycle length sits in the 8-12 week window with a 2-4 week washout.
Sermorelin is dosed differently because of its half-life. The historical clinical use of sermorelin in adults was a once-daily subcutaneous injection at bedtime to align with the natural nocturnal GH pulse. The diagnostic dose was 1 mcg/kg intravenously; the paediatric therapeutic dose was approximately 30 mcg/kg subcutaneously at bedtime. Adult wellness-clinic protocols since the discontinuation of Geref typically use a flat 200-500 mcg subcutaneous dose at night through compounding pharmacies, though research-published doses for adult sermorelin monotherapy outside paediatric GH deficiency are limited and not standardised.
Evidence: what the studies actually show#
There is no head-to-head randomised trial comparing ipamorelin and sermorelin in adults on a body-composition or longevity endpoint. The evidence base for each runs on a parallel track.
For ipamorelin, the strongest human data sits in postoperative ileus. The 2014 Beck et al. Phase II trial administered intravenous ipamorelin at 0.03 mg/kg twice daily in bowel-resection patients. Earlier animal work has shown that a single dose of ipamorelin at 1 mg/kg decreased time to first bowel movement in a rat postoperative ileus model, and repetitive dosing of 0.1 or 1 mg/kg significantly increased cumulative fecal pellet output, food intake, and body weight gain, suggesting postsurgical infusions may ameliorate symptoms in patients with postoperative ileus . None of this is a body-composition study. The GH-release evidence in healthy subjects is dose-ranging pharmacology, not outcome trials.
For sermorelin, the FDA-era evidence base is larger because the molecule had a registered indication. In clinical studies the incidence of hypothyroidism during sermorelin therapy was 6.5%, and in the largest clinical study 8 of 110 enrolled patients were on thyroid replacement therapy prior to sermorelin therapy with an additional 5 starting after initiating therapy , per the RxList sermorelin acetate label. Paediatric data showed measurable height-velocity gains in GH-deficient children. Adult longevity data is the gap that every honest sermorelin review names: definitive research to support the anti-aging effect of sermorelin is lacking, and use in healthy adults to reverse the effects of aging remains controversial .
Net read: sermorelin has the longer regulatory paper trail; ipamorelin has the cleaner mechanistic story; neither has a published adult head-to-head on body composition.
Side effects and contraindication profile#
The two profiles converge on the trivial end and diverge in interesting ways at the edges.
Injection-site reactions dominate both. Injection site reactions are by far the most common sermorelin side effect, affecting roughly 1 in 4 to 1 in 3 users at some point during their protocol . Ipamorelin produces similar local reactions at similar rates because the route is identical (subcutaneous, insulin syringe, abdominal or thigh fat pad).
The diagnostic-use intravenous sermorelin label flags a specific symptom cluster. When administered intravenously for diagnostic use, the following adverse reactions have been noted: flushing of the face, injection site pain, redness and/or swelling, nausea, headache, vomiting, dysgeusia, pallor and tightness in the chest . The subcutaneous adult dose is gentler, but flushing and headache still appear at low single-digit frequencies.
Where ipamorelin pulls ahead is endocrine cleanliness. Preliminary evidence and the swine-model work cited above show no measurable change in cortisol, prolactin, ACTH, FSH, LH, or TSH. Sermorelin can unmask subclinical hypothyroidism (the 6.5% rate in the original label is not nothing) and has been associated with mild fluid retention in early weeks. Both peptides carry the same hard contraindication: active or recent malignancy, because elevated IGF-1 is a permissive growth signal.

When to choose ipamorelin#
- You want flexibility on dosing time. The 2-hour half-life supports morning, post-workout, or pre-bed shots without disrupting the nightly GH pulse.
- You are sensitive to cortisol or prolactin shifts. Research has shown ipamorelin leaves those axes essentially untouched, which matters if you are tracking HPA-axis biomarkers.
- You plan to stack with a GHRH analog like CJC-1295 (no DAC). Ipamorelin is the canonical GHRP partner in that combination, and the paired effect on both receptor families is supra-additive on GH output.
- You want micro-dose control. Dosing in mcg with insulin syringes lets you titrate in 50 mcg steps, which sermorelin's 200-500 mcg adult range does not match.
When to choose sermorelin#
- You want the molecule with the deepest regulatory paper trail. FDA approval history, a published diagnostic dose, and decades of compounding-pharmacy use give clinicians a more familiar framework.
- You are optimising for sleep and the natural nocturnal GH surge. The short pulse aligns cleanly with the first slow-wave sleep cycle when injected at bedtime.
- You want to preserve the somatostatin negative feedback loop intact. Sermorelin's clearance is so fast that pituitary feedback control is essentially undisturbed, which has been shown to make supraphysiologic stacking accidents harder to produce.
- You want a single nightly shot and find multiple daily injections impractical.
Can you stack them?#
You can, and historically clinics did, but it is the older protocol. The modern equivalent replaces sermorelin with CJC-1295 (no DAC, also called Mod GRF 1-29) because the latter has longer functional duration at the GHRH receptor while keeping the same mechanism. Stacking sermorelin and ipamorelin together is mechanistically valid (GHRH receptor plus ghrelin receptor on the same somatotroph fires a larger pulse than either alone) but logistically clumsy because sermorelin's 12-minute half-life forces co-injection at every ipamorelin dose. Most current research-published stacks have moved on for that reason. If you are choosing a single agent rather than a stack, the comparison below stays clean.
Verdict#
For most adult readers approaching the GH axis for the first time, sermorelin is the better starting point because it has the longer human safety record and the regulatory paper trail that makes clinical conversations easier. For readers who already understand peptide injection mechanics, want daytime dosing flexibility, plan to stack with a long-acting GHRH analog, or are specifically trying to avoid any cortisol or prolactin shift, ipamorelin is the better fit. Neither is the universally correct answer. The deciding factors are your dosing tolerance (one nightly shot versus two-or-three daily), your stacking intent, and which receptor side of the GH axis your protocol design favours.
If you are trying to decide on a number rather than a vibe, run your IGF-1, fasting glucose, and morning cortisol first. The peptide that fits your bloodwork is the one to start with.
Run your bloodwork before you run the protocol#
The ipamorelin versus sermorelin question is the right question to ask second. The first one is whether your IGF-1, fasting glucose, and morning cortisol actually point at the GH axis at all. Klarovel does not sell or stock peptides; research-grade ipamorelin and sermorelin are available from specialised suppliers. What Klarovel does is help you quantify which peptide your numbers point to before you spend a cycle finding out the hard way. Run the peptide calculator to size the dose to your weight and goal, walk through the questionnaire to map your baseline against the two protocols, or read how Klarovel works to see where the protocol layer ends and the supplier layer begins.
Frequently asked questions
Keep reading

Epitalon vs NAD+: Which Longevity Path Fits You (2026)
Epitalon activates telomerase on short cycles; NAD+ precursors refill a daily metabolic cofactor. Head-to-head on evidence, dosing, and how to choose.
BPC-157 vs Thymosin Alpha-1: Healing vs Immune Modulation (2026)
BPC-157 targets tissue repair and gut lining; thymosin alpha-1 modulates T-cell immunity. Head-to-head on mechanism, dosing, side effects, and stacking.

MK-677 vs Tesofensine: GH Support vs Fat Loss (2026)
MK-677 raises GH and appetite; tesofensine is a central appetite suppressor with 9% weight loss. Head-to-head on mechanism, dose, and evidence.