
Most peptide users default to a single comfortable injection spot and stay there for months. That choice quietly shapes absorption, comfort, and the long-term health of the tissue under the needle. This guide walks through the four practical subcutaneous zones, what each does to pharmacokinetics, and how to rotate without thinking about it.
Key takeaways#
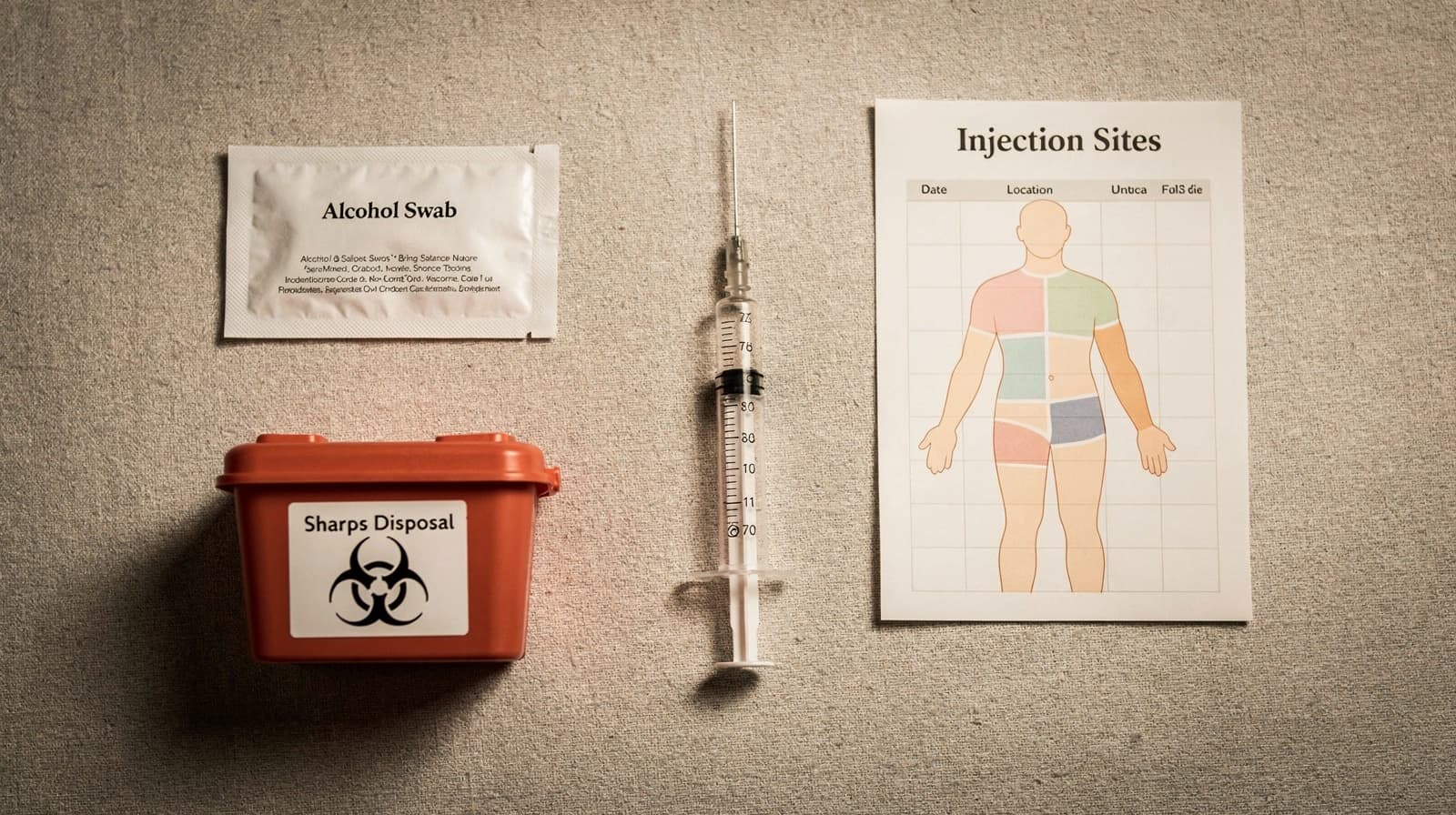
- The four standard subcutaneous zones for peptide injections are the abdomen, the anterior or outer thigh, the back of the upper arm, and the deltoid region of the shoulder.
- Abdominal injection generally produces faster and higher peak plasma concentrations than thigh or arm sites for many peptides and proteins, while total exposure (AUC) is often comparable.
- Incorrect site rotation is the single strongest documented risk factor for lipohypertrophy, the rubbery lump that distorts absorption over time.
- Each zone has a usable area of several square inches; spacing injections at least 2-3 cm apart inside a zone, and waiting weeks before reusing the exact spot, is what actually protects tissue.
- Site choice should match the peptide goal: faster onset and predictable weekly levels favour the abdomen; slower, steadier release favours thigh or buttock.
Why the injection site matters more than most users think#
Peptides and proteins do not behave like small-molecule pills. Subcutaneous absorption depends on local blood flow, lymphatic drainage, fat thickness, and tissue health. A 2021 ScienceDirect review of FDA bioavailability data found that some subcutaneously administered therapeutic proteins and peptides such as insulins, human growth hormone, and monoclonal antibodies exhibit a different extent and rate of absorption when administered from distinct injection sites . That same survey covered 19 immunoglobulin G antibodies, 18 peptides and small proteins under 16 kDa, and 8 non-IgG proteins with clinical pharmacokinetic data from multiple subcutaneous injection sites , making it one of the better cross-product datasets available.
Research suggests that the practical effect of site selection varies by molecule. For insulin and many short peptides, the abdomen wins on speed. For modern GLP-1 receptor agonists, site differences are smaller in clinical practice. The principle stays the same: pick a site that matches the goal, rotate it on a schedule, and check the tissue.
The abdomen is the fastest and most forgiving site#
The abdomen is the most studied subcutaneous zone. It offers a thick, even fat layer, dense capillary supply, and enough surface area for months of rotation. According to UK pharmacy guidance, the abdomen should be injected at least 5 centimetres (about two inches) from the navel, avoiding the area directly around the belly button and the waistline where clothing may rub.
Pharmacokinetic studies have shown a measurable speed advantage. A classic 1982 Diabetologia trial reported that insulin was absorbed faster from the abdomen than from the thigh under resting conditions and during exercise. A later review summarised by the Journal of Diabetes Research found that injection into the abdominal region produced greater and earlier peak concentrations than the deltoid and thigh in healthy subjects, with the time to maximum plasma concentration after abdominal injection being less than half that of the two other sites, and Cmax reduced by 32% in the thigh and 42% in the deltoid . In people with diabetes, Cmax has been reported to be 28% higher and occur more than twice as fast upon injection of human insulin into the abdomen compared to the thigh .
What this means in practice: if a peptide protocol calls for predictable weekly peaks (GLP-1 agonists, GH secretagogues), the abdomen is the default starting zone. Stay outside the 5 cm peri-umbilical ring, keep injections at least one finger-width apart, and use the left and right sides as separate quadrants.

The thigh is the slower, steadier alternative#
The anterior and outer thigh is the second most common zone, mainly because it is easy to self-inject and easy to see. Skin and fat thickness are slightly lower than the abdomen, and blood flow is lower at rest. A 2022 needle-free insulin study measured skin thickness of 2.45 mm at the abdomen, 2.18 mm at the upper arm, and 1.93 mm at the thigh, with a significant difference between abdomen and thigh.
That lower perfusion translates to slower absorption. Norwegian and Danish protocol guidance for insulin has long noted that absorption from subcutaneous thigh tissue is slower than from the abdominal wall, a finding confirmed in a randomised trial in type 1 diabetes that compared subcutaneous abdominal, subcutaneous thigh, and intramuscular thigh injection of soluble insulin. For peptides where a sharp peak is the goal, the thigh is the wrong default. For peptides where a longer, gentler release is preferred, or where evening dosing should not produce sudden side effects, the thigh is associated with smoother kinetics.
Anatomically, the usable zone runs from roughly four finger-widths above the knee to four finger-widths below the groin crease, on the outer front of the thigh, avoiding the inner thigh where larger vessels run closer to the surface.
The upper arm gives an intermediate profile, with caveats#
The back of the upper arm (triceps region) sits between abdomen and thigh in most pharmacokinetic surveys. It has thinner subcutaneous fat than the abdomen in many people, especially in lean users, so a pinch technique becomes essential to avoid intramuscular delivery. Preliminary evidence from needle-free insulin work showed no significant difference in glucose infusion rate area under the curve between abdomen, upper arm, and thigh, so for some compounds the arm performs as a reasonable abdominal substitute.
The two practical problems with the upper arm are self-access and fat depth. Self-injecting the back of the contralateral arm is awkward; many users rely on a partner or lean against a chair to pivot the arm forward. In leaner users, the available pinch may be less than 1 cm, which raises the risk of inadvertent intramuscular delivery and a faster, less predictable response.
A 2023 Phase 1 study on lenacapavir, a long-acting subcutaneous antiretroviral, enrolled ten participants each into thigh, upper arm, and abdomen cohorts to compare pharmacokinetics across body sites. That kind of head-to-head data is rare, but it points to the same pattern: the arm sits in the middle, and when fat depth is adequate, it is a defensible rotation target.
The deltoid and shoulder are niche, not default#
The deltoid is sometimes lumped together with "upper arm" but anatomically refers to the rounded shoulder muscle, not the triceps. For most peptides, the deltoid is not a standard self-administered subcutaneous site. Subcutaneous fat over the deltoid is usually thin; the underlying muscle is close to the skin; and the risk of intramuscular delivery is meaningful. The insulin pharmacokinetic literature consistently pairs "deltoid" with slower, less consistent absorption when used as a subcutaneous site, with one analysis showing a 42% reduction in Cmax compared to abdominal injection.
Where the deltoid does appear is in industry protocols for specific drug products. Insulin lispro studies have used the abdominal wall, thigh, and deltoid as the three comparison sites for pharmacokinetic equivalence work. For most peptide users, the practical rule is simpler: use the back of the upper arm (triceps), not the rounded shoulder, and reserve true deltoid injection for IM-formulated products administered by a clinician.

Rotation is the single highest-impact habit#
If only one habit is taken from this guide, it should be structured rotation. The evidence is unusually clear. A Spanish study of 430 insulin-injecting outpatients found that nearly two-thirds (64.4%) had lipohypertrophy, and of those who rotated sites correctly, only 5% had lipohypertrophy, while 98% of those with lipohypertrophy either did not rotate or rotated incorrectly. A 2025 systematic meta-analysis of 51 studies has shown that the strongest contributor to lipohypertrophy was incorrect injection site rotation, with a pooled odds ratio of 8.85, followed by needle reuse at 3.20.
Lipohypertrophy is not cosmetic. It changes how the next injection is absorbed. Studies have shown that injection into lipohypertrophied tissue produced a 25% decrease in insulin Cmax and a 22% decrease in 4-hour exposure compared to injection into normal abdominal tissue. For a weekly GLP-1 or growth hormone peptide, that variability is enough to make a protocol feel inconsistent without any obvious cause.
A workable rotation rule for most users:
- Divide each zone into a grid (four quadrants per side of the abdomen, three bands on each thigh, two bands on each upper arm).
- Use a new quadrant or band every injection, working clockwise through the available sites.
- Wait at least four weeks before reusing the exact same point.
- Inspect every site weekly by sight and by gentle palpation. Lumps, hardness, or persistent redness are signs to stop using that area for at least two to three months.
A practical schedule lives in the Klarovel peptide calculator, which can prompt a rotation reminder alongside the dose log.
Comfort and absorption depend on temperature and technique#
Site choice is necessary but not sufficient. Two technique details have outsized effects on pain and absorption.
First, temperature. Cold peptide injected straight from a refrigerator constricts local capillaries, increases sting, and may briefly slow uptake. Letting the vial sit at room temperature for 15-20 minutes before drawing makes the injection more comfortable without risking peptide degradation for properly reconstituted compounds. The same applies to alcohol swab residue: let the skin air-dry fully before insertion.
Second, depth. Most modern insulin pens use 4-6 mm needles, and most peptide users are best served by similar lengths with a gentle pinch. The pinch matters more than the angle. In lean users, a 45-degree angle with a firm pinch is safer than a 90-degree perpendicular insertion. The goal is to deposit the peptide into adipose tissue, not muscle, where absorption becomes faster but more erratic. Preliminary evidence from insulin-related work suggests that the absorption rate is known to be a lot quicker when insulin is injected into a muscle than when injected into fat tissue, which is exactly what a weekly SC protocol is trying to avoid.
For a deeper walkthrough of needle gauge, reconstitution volume, and angle selection, see the companion guide on how the Klarovel protocol layer works and the broader Klarovel disclosures page for the limits of wellness-grade guidance.
A protocol is only as good as the spot it lands in#
Peptide outcomes are usually attributed to the molecule. In practice, they are shaped just as much by where the needle goes and how often that spot has been used before. Pick a zone that matches the goal, rotate on a schedule, inspect the tissue weekly, and the protocol does what it was designed to do. Site selection is one piece of what peptide therapy involves. Build the rotation map into the dose log from day one with the Klarovel peptide calculator, and create a Klarovel account to keep that map consistent across the cycles ahead.
Frequently asked questions
Keep reading
Peptide Injection Technique: A Research Skills Primer
How to think about peptide injection technique: site selection, angle, needle gauge, rotation, and sterility. A research-grade primer for protocol literacy.

How to inject peptides: technique, sites, rotation
How to inject peptides subcutaneously in 2026. Insulin syringe choice, four primary sites, rotation discipline, the 5-10 second hold, and the Norway frame.
Bacteriostatic water: why it matters and how much to use
Bacteriostatic water is the 0.9% benzyl-alcohol diluent that keeps reconstituted peptides stable for 28 days. Here's the chemistry, the volumes, and the math.