Most peptide-protocol failures are not pharmacology failures. They are technique failures: a needle placed too deep, a site reused until the tissue scars, a vial swabbed with a dry alcohol pad. This primer covers what the subcutaneous-injection literature actually shows about angle, gauge, rotation, and sterility, and how a researcher should translate that into a repeatable handling protocol.
Key takeaways#
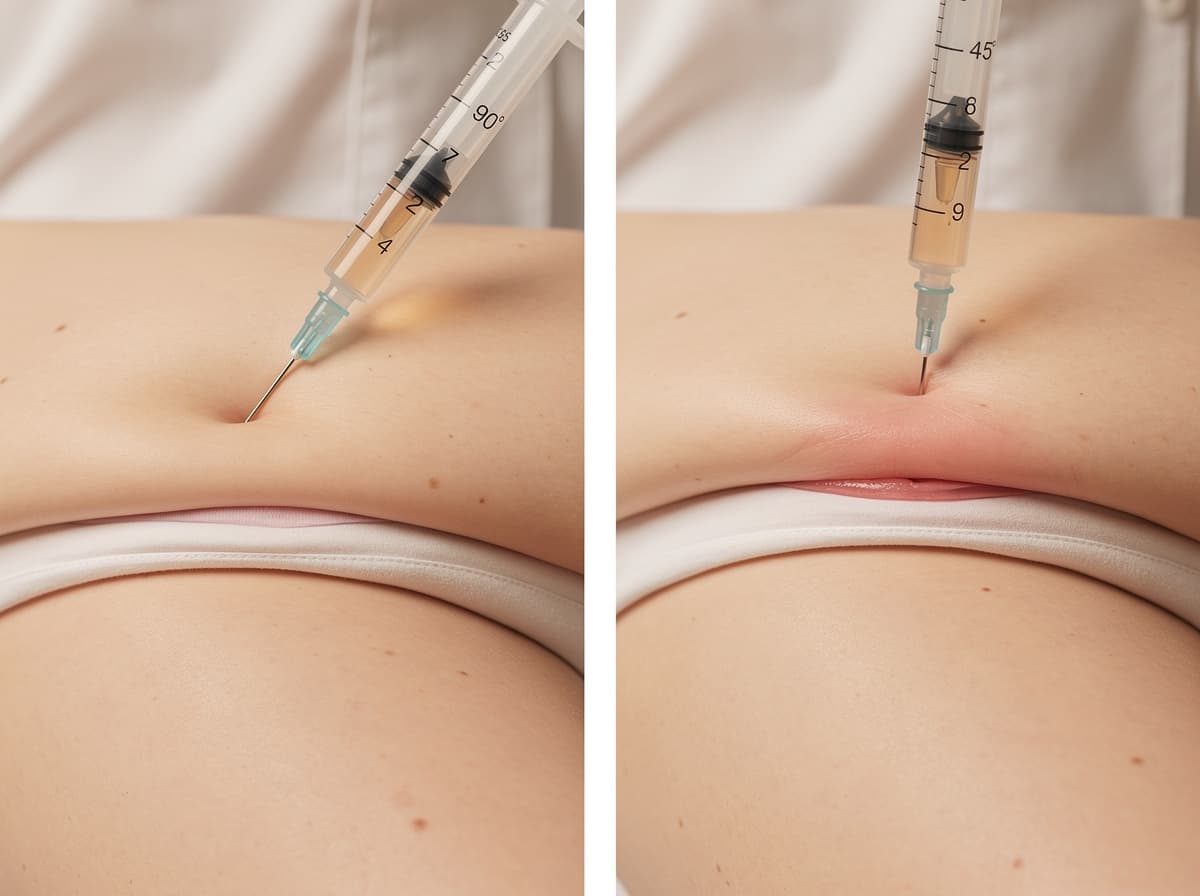
- Subcutaneous injection angle is dictated by tissue depth, not preference: 90° when a 2-inch skinfold is easy to pinch, 45° when only ~1 inch can be grasped.
- Needle length matters more than gauge for depth control. Most subcutaneous workflows use 4-6 mm pen needles or 5/16"-1/2" insulin syringes at 28-31 G.
- Lipohypertrophy (firm, rubbery subcutaneous nodules) is the single most predictable long-term complication of repeated injections into the same spot, and rotation across a postcard-sized area is the most evidence-supported countermeasure.
- Massaging the site after withdrawal is discouraged; it can change absorption kinetics and contribute to bruising.
- Sharps must be disposed of in a rigid, puncture-resistant container, never recapped, never in household trash.
Why injection technique is a protocol-literacy issue, not a clinical one#
Klarovel does not sell, source, or fulfil peptides. How a researcher handles research-grade material in a self-administered or laboratory setting determines whether the protocol layer (timing, dose-spacing, cycle structure) means anything at all. If absorption is erratic because the same square inch of abdominal tissue has been hit forty times, the elegance of the dosing schedule is irrelevant.
The subcutaneous (SC) route is the standard for most peptide research because it deposits material into the adipose tissue layer beneath the dermis, where blood flow is low and absorption is slow and sustained. Open educational sources on SC injection note that this tissue has few blood vessels, so substances administered via this route show a slow, sustained rate of absorption, which is why peptide pharmacokinetics behave so differently from oral or intramuscular routes.
Research has shown that injection-technique errors, not formulation errors, account for a large share of inconsistent outcomes in chronic SC injection populations. The diabetes literature is the closest analogue (decades of data, millions of patients) and it has consistently associated poor technique with measurable absorption variability.
Angle, gauge, and depth: the three variables that decide where the peptide ends up#
The clinical consensus on subcutaneous injection angle is well documented. Nursing-skills references state that a 45- or 90-degree angle is used for a subcutaneous injection, with the steeper angle for normal or higher-BMI subjects and the shallower angle for thin individuals with less adipose tissue. The practical rule that has been shown to work across body types: if a 2-inch skinfold can be pinched between thumb and forefinger, 90° is appropriate; if only about 1 inch can be grasped, 45° lowers the risk of inadvertently depositing into muscle.
Needle length is the variable most researchers underweight. Manufacturer guidance from Lilly's subcutaneous injection reference indicates that needles 6 mm or less are recommended in most cases, and that 4-5 mm needles can deliver SC contents at 90° without a skinfold in many subjects. Longer needles (8 mm and above) generally require a skinfold and/or a 45° angle to limit the risk of depositing too deeply. Gauge (28 G, 29 G, 30 G, 31 G) influences pain and back-pressure on the syringe plunger; it does not change depth. Thinner gauges hurt less but bend more easily if the injection is rushed.
Volume is the third constraint. SC volumes are typically capped at 1 mL per site in adults; larger volumes have been associated with poor absorption and additional discomfort. If a research protocol calls for more than 1 mL, splitting into two sites is the convention.
Site selection and rotation: the most under-rated determinant of consistent absorption#
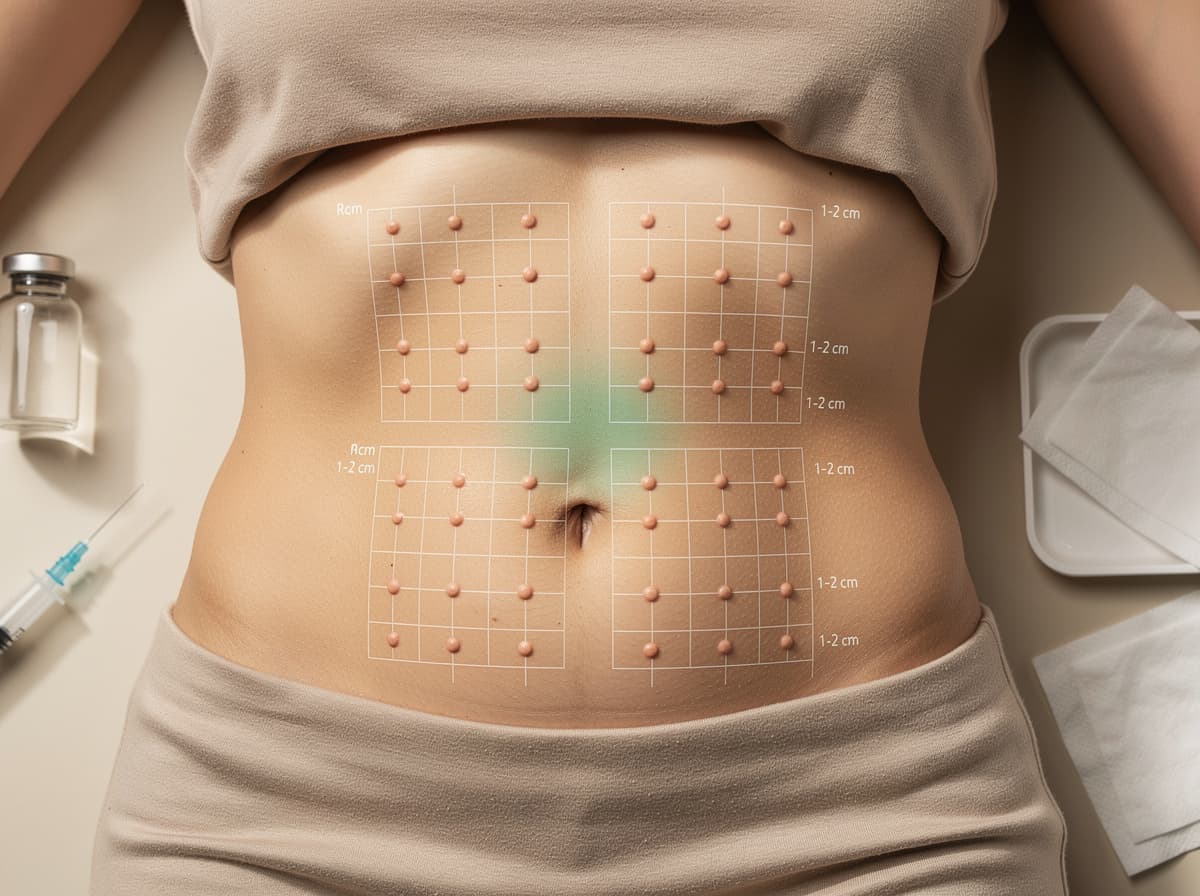
The standard SC sites are the abdomen (avoiding a ~5 cm radius around the navel), the outer aspect of the upper thigh, and the back of the upper arm. Absorption speed varies by site: the American Diabetes Association has noted that the body absorbs material fastest from the abdomen, less quickly from the arm, and slowest from the buttocks and thighs. For a research user trying to keep pharmacokinetics consistent across a cycle, this means picking one anatomical region and rotating within it, rather than alternating between abdomen and thigh and confounding the variability of the compound with the variability of the site.
The rotation evidence is unambiguous. A study cited in Frontiers in Endocrinology found that people who rotated within an area the size of a credit card were 23.2 times more likely to develop lipohypertrophy than those who used a postcard-sized area. A separate Diabetes Technology Society review reports that almost half of insulin users have been found to have lipohypertrophy, and that common risk factors are failure to rotate sites, concentrating injections in a small area, and needle reuse. The same review notes that areas with injection-induced lipohypertrophy contain a significantly larger number of macro-adipocytes and fibrosis, which is why absorption from those sites becomes unpredictable.
A workable rotation scheme:
- Divide the chosen region (e.g., abdomen) into four quadrants.
- Space successive injections by at least 1-2 cm (one finger width).
- Use one quadrant per week, then advance.
- Log each site (paper, calendar, or app) so you do not rely on memory.
- Visually inspect and palpate sites weekly for firmness, dimpling, or rubbery nodules.
Research suggests that structured rotation training measurably reduces lipohypertrophy incidence: a quasi-experimental study published in ScienceDirect reported a significant reduction in lipohypertrophy incidence and grade at 6-month follow-up after an ameliorated site-rotation intervention. Preliminary evidence from the same literature also points to needle reuse as an independent driver of tissue change, which is why single-use is the standard.
The aseptic sequence: a step list that survives contact with reality#
Aseptic technique is not theatre. It is the sequence that keeps the bioburden on the needle, the stopper, and the skin low enough that the SC tissue can clear it without local inflammation. The skeleton of the sequence, distilled from open nursing references and pharmaceutical manufacturer documentation:
- Hand hygiene. Soap and running water for at least 30-60 seconds, then dry on a clean disposable towel.
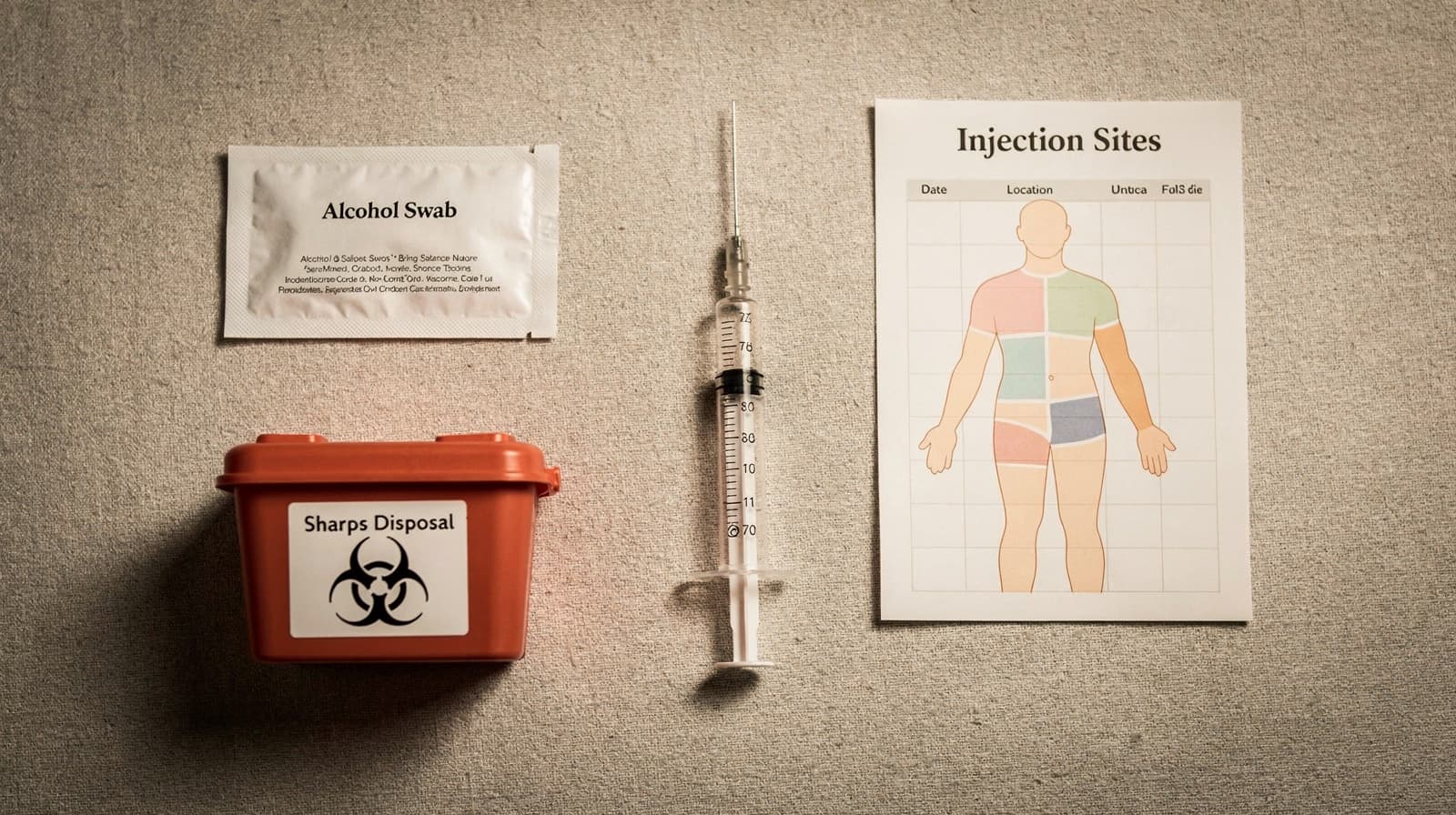
- Surface setup. Clean a hard, non-porous surface. Lay out: vial, syringe, two alcohol swabs (70% isopropyl), gauze, sharps container.
- Vial preparation. Swab the rubber stopper with alcohol; allow it to dry. Drawing through a wet stopper has been associated with stinging and skin irritation at the injection site.
- Draw and inspect. Draw the prescribed volume. Tap and expel large air bubbles. Confirm the volume against the syringe markings.
- Site preparation. Select a site at least 1-2 cm from the previous one, outside any palpable nodule. Swab in a firm circular motion, then let the skin dry fully. Inserting into wet alcohol is uncomfortable and may introduce alcohol into the tissue.
- Insertion. Pinch (if needed), insert at the correct angle in a single smooth motion, release the pinch, then depress the plunger steadily.
- Withdrawal. Remove the needle at the same angle. Apply gentle pressure with sterile gauze. Open-source nursing protocols state explicitly: do not massage the site.
- Disposal. Engage the safety shield if present. Place the entire syringe-needle unit, uncapped, into a rigid puncture-resistant sharps container. Never recap, never re-use, never throw into household waste.
- Log. Record date, site quadrant, volume, lot if relevant, and any local reaction.
Studies have shown that even modest training on this sequence (structured injection-technique education) reduces measurable complications. The point is not perfection on any single dose; the point is repeatability across hundreds of doses.
A clean technique is the silent variable behind every clean protocol#
The peptide-research community spends enormous attention on dose, timing, and stacking. It spends far less on the mechanics of getting the compound into tissue consistently. The literature is clear that technique variance, not compound variance, is often the larger source of noise in a self-administered protocol. Match the angle to the tissue, rotate across a postcard-sized field, keep the sequence sterile, and log every site. Then, and only then, can the protocol layer be evaluated honestly, as part of the broader picture of what peptide therapy involves.
To plan a cycle around a repeatable technique baseline, register a free Klarovel account, use the peptide calculator to lock dose math before the first injection, and review how Klarovel works for the full research-context framing.
Frequently asked questions
Keep reading

Peptide Injection Sites: A Site-by-Site Protocol Guide
A site-by-site review of abdomen, thigh, upper arm, and shoulder for peptide injections, with pharmacokinetic differences and rotation rules that protect tissue.

How to inject peptides: technique, sites, rotation
How to inject peptides subcutaneously in 2026. Insulin syringe choice, four primary sites, rotation discipline, the 5-10 second hold, and the Norway frame.
Bacteriostatic water: why it matters and how much to use
Bacteriostatic water is the 0.9% benzyl-alcohol diluent that keeps reconstituted peptides stable for 28 days. Here's the chemistry, the volumes, and the math.