The BPC-157 + TB-500 combination is the most frequently researched healing-peptide stack. The mechanism rationale is sound: complementary pathways for tissue repair, covering angiogenesis, fibroblast migration, cell migration, and anti-inflammatory effects. What the stack doesn't have is clinical trial evidence directly comparing it to either peptide alone.
Why people call it the wolverine peptide stack#
The "wolverine peptide" nickname did not come from a clinical paper. It came from forum communities (sports-injury subreddits, research-use boards, recovery-focused podcasts) reaching for a shorthand for the rapid-recovery angle observed in animal models of BPC-157 and TB-500. The nickname stuck because the preclinical literature on the stack reads, at a glance, like a recovery cheat code: faster collagen deposition, broader cell migration, anti-inflammatory effects across multiple tissue types. Hence "wolverine peptide stack", a reference to the comic-book character known for accelerated healing.
The honest framing is narrower. Research has shown promising preclinical results for each peptide individually, and mechanism-level reasoning suggests the wolverine peptide combination covers complementary repair pathways. What it has not shown is a head-to-head clinical trial against either peptide alone in the same human injury population. The "wolverine stack peptide" name compresses real biology and real evidence gaps into one word, which is how nicknames work but not how protocol decisions should be made. Use the nickname for shorthand; weigh the protocol on the published evidence below.
Why stack them at all#
The stacking argument rests on complementary, not redundant mechanisms. BPC-157 works primarily through VEGFR2-driven local angiogenesis and fibroblast mobilisation at the injury site. TB-500 works primarily through actin binding and is associated with broad cell migration (immune cells, fibroblasts, stem cells, endothelial cells) systemically.
In practice, tissue repair after a significant injury is not a single-mechanism process. It involves:
- Haemostasis (clotting) → early
- Inflammation → hours to days
- Proliferation (fibroblast and endothelial cell migration, new tissue formation) → days to weeks
- Remodelling (collagen organisation, maturation) → weeks to months
BPC-157 acts strongly during the proliferation phase at the local site. TB-500 acts across the inflammation and proliferation phases systemically. A stack that uses both is attempting to cover both the local-site intensity and the systemic cell-mobilisation breadth.
This is mechanism-plausible, not clinical-trial-proven. The distinction matters.
What the evidence actually shows#
For BPC-157 alone: systematic reviews of preclinical data consistently report accelerated healing across tendon, ligament, muscle, bone, and GI mucosal injury models, with related entries indexed in PubMed. Research has shown the effect across animal injury models is robust, but human clinical evidence is limited to three small open-label pilot studies. No Phase 3 trial exists.
For TB-500 alone: preclinical evidence for cardiac, dermal wound, muscle, and stroke recovery. Human clinical evidence is even thinner than for BPC-157.
For the BPC-157 + TB-500 combination: no published clinical trial has directly compared the stack to either peptide as mono-therapy in the same injury population. The "stack works better than mono" claim is derived from:
- Mechanism complementarity (scientifically reasonable)
- Aggregated case-series reporting from sports-medicine and research-use communities
- Some preclinical models where sequential or combined use has been shown to produce additive effects
This is a real evidence base, but it's weaker than the evidence for either peptide as mono-therapy. Honest framing: the stack is likely to be better, and almost certainly not worse, than either peptide alone, but the clinical-trial data to prove it doesn't exist yet.
The dosing framework#

Typical stacked-protocol structure:
BPC-157 component#
- Dose: 250–500 mcg per injection
- Frequency: 1× daily (simpler) or 2× daily (more aggressive)
- Route: subcutaneous, prefer near injury site
- Cycle length: 4–8 weeks
TB-500 component#
- Loading phase: 2–2.5 mg once weekly for 4–6 weeks
- Maintenance phase: 2 mg every 2–4 weeks for weeks 7–12
- Route: subcutaneous, any site
- Total cycle length: 8–12 weeks (matches or slightly exceeds BPC-157 cycle)
The two components run in parallel. Daily BPC-157 injections alongside weekly TB-500 injections. Some protocols combine both peptides into a single syringe; others keep them separate. Neither approach shows clear superiority in preclinical data.
Reconstitution math: a 5 mg BPC-157 vial + 2 mL BAC water = 2,500 mcg/mL (a 250 mcg dose = 10 units). A 5 mg TB-500 vial + 2 mL BAC water = 2.5 mg/mL (a 2 mg dose = 80 units). The Klarovel peptide calculator handles both. For schedule planning, the titration calculator builds the week-by-week view.
The blend question#
Klarovel does not sell, source, or fulfil peptides; how you obtain BPC-157 and TB-500, in vial or pen form, is outside the platform. A combination blend product, sometimes marketed as "Wolverine" in research-use circles, combines both peptides into a single vial. Pre-blended products offer dosing simplicity (one injection vs two) at the cost of fixed peptide ratios that may not match every use case.
For most research protocols, separate vials are more flexible: you can change the BPC-157 frequency, pause one while continuing the other, or adjust ratios based on injury phase (more BPC-157 early, more TB-500 sustained).
Injury-phase dosing variations#
Some research protocols vary the stack composition across injury phases:
Acute phase (first 2 weeks post-injury):
- BPC-157: 500 mcg twice daily (higher frequency)
- TB-500: 2.5 mg once weekly (full loading dose)
Proliferation phase (weeks 3–6):
- BPC-157: 250–500 mcg once daily (sustained)
- TB-500: 2 mg once weekly (continued loading)
Remodelling phase (weeks 7–12):
- BPC-157: taper off or stop
- TB-500: 2 mg every 2–4 weeks (maintenance)
This phase-varying approach matches the biology of tissue repair but is more complex to schedule. For simpler protocols, constant dosing through the full cycle works, the stack is forgiving.
Safety in a stack context#
Both peptides have benign short-term safety profiles individually. Combining them does not introduce a known new risk at typical research-use doses. Reports of stack-specific adverse effects are rare and typically consistent with the known individual profiles (injection-site irritation, mild transient fatigue).
The shared contraindications apply:
- Active or recent malignancy
- Pregnancy or breastfeeding
- Under 21
- Active anticoagulation therapy (theoretical concern based on BPC-157's vascular effects; not well characterised)
How to decide whether to stack#
Three questions filter the stack decision:
- Is the injury multi-component? Sports injuries involving tendon + muscle + connective tissue, post-surgical recovery, or chronic overuse injuries benefit more from broad mechanism coverage. Isolated tendon strain with no other tissue involvement may be fine on BPC-157 alone.
- Is the goal acceleration or broad support? Stacks are more useful for comprehensive support. For a single targeted mechanism (e.g., gastric mucosa healing), mono-therapy is appropriate.
- Is budget a factor? The stack roughly doubles peptide consumption over a 12-week cycle. For cost-sensitive protocols, mono-therapy is reasonable; for comprehensive-coverage protocols, the stack cost is typically justified by the multi-mechanism logic.
For anyone considering a research-use stack, Klarovel's questionnaire maps injury type and contraindications to recommendations. The BPC-157 guide, TB-500 guide, and BPC vs TB comparison provide the individual context, and the broader peptides for healing overview places the stack within the full tissue-repair toolkit. The peptide calculator handles dose math.
The BPC-157 + TB-500 stack is the most reasonable multi-peptide tissue-repair protocol in the research-use toolkit. It's not a magic combination. It's a well-reasoned application of complementary mechanisms, with the caveat that the clinical evidence is still catching up to the mechanism.
Frequently asked questions
Keep reading
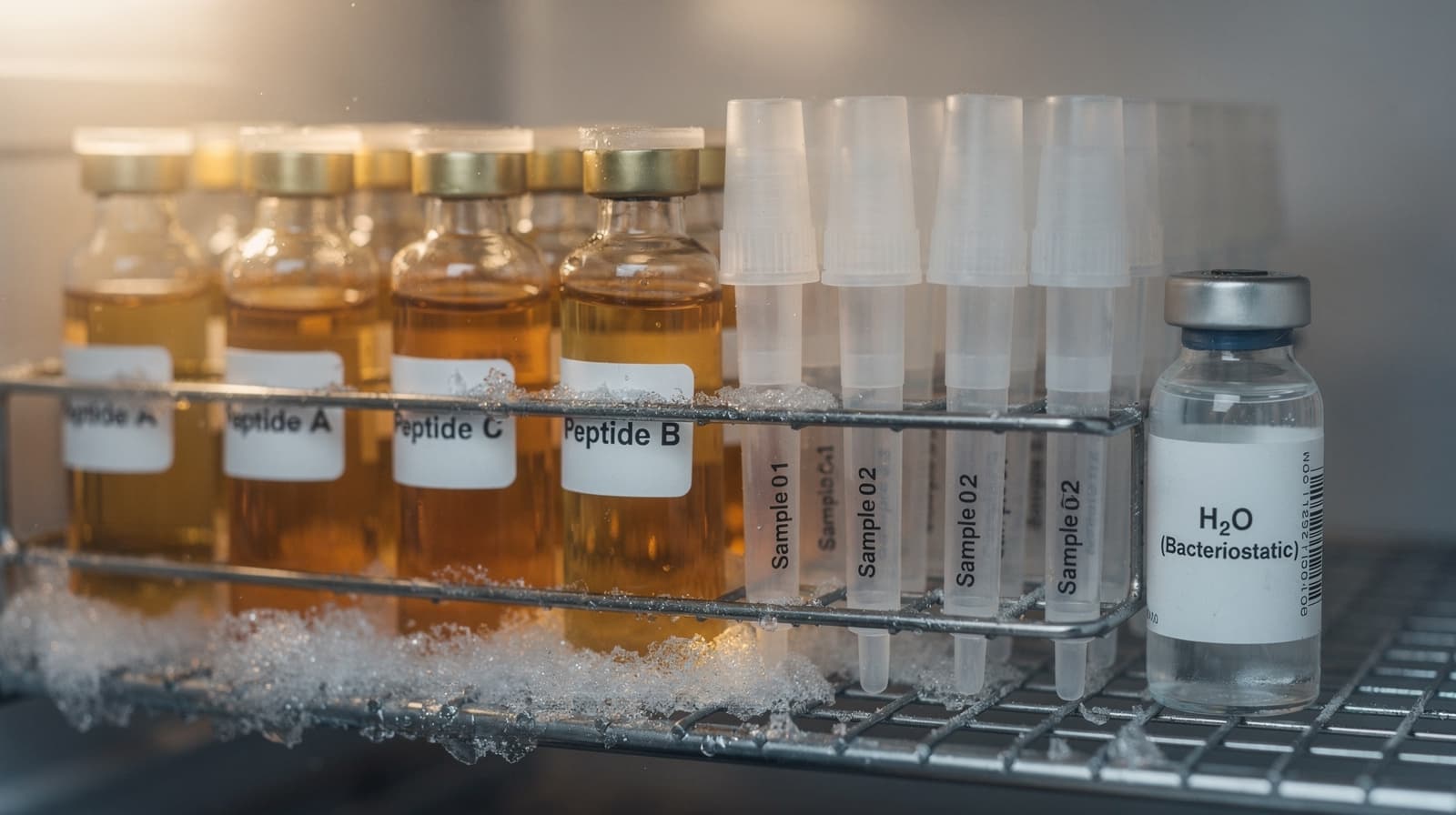
Peptide Storage Guide: Cold Chain, Aliquots, Shelf Life
How to store lyophilized and reconstituted research peptides: freezer temperatures, aliquoting workflow, bacteriostatic water windows, and cold-chain rules.

Peptide Injection Sites: A Site-by-Site Protocol Guide
A site-by-site review of abdomen, thigh, upper arm, and shoulder for peptide injections, with pharmacokinetic differences and rotation rules that protect tissue.
Peptide Injection Technique: A Research Skills Primer
How to think about peptide injection technique: site selection, angle, needle gauge, rotation, and sterility. A research-grade primer for protocol literacy.