
The question "do any peptides help with ADHD?" sits in an uncomfortable gap. Stimulant shortages are real, adult diagnoses are climbing, and yet the peptide answer is more interesting than the wellness internet usually admits. This piece walks through what Semax, Selank, and BDNF-modulating peptides have actually shown in the literature, what they have not, and how to read the Russian clinical record without losing scientific footing.
Key takeaways#
-
An estimated 15.5 million U.S. adults (6.0 percent) have a current ADHD diagnosis, bringing the combined adult-and-child total to roughly 22 million people.
-
Semax is the only peptide with a published hypothesis paper proposing it as a candidate for ADHD, grounded in dopamine and BDNF mechanisms.
-
Intranasal Semax at 50 and 250 micrograms per kilogram has been shown to produce a rapid increase in BDNF protein in the basal forebrain within three hours in rats.
-
Selank targets anxiety and GABAergic tone, not attention per se, but it is often misdescribed as an "ADHD peptide" in consumer marketing.
-
No peptide is FDA- or EMA-approved for ADHD. Western randomised trials in ADHD populations remain absent.
ADHD demand is outrunning the stimulant supply#
The interest in peptides for attention is partly a story about supply. The CDC found that 71.5% of adults taking a stimulant medication had difficulty getting their ADHD prescription filled in the previous 12 months, and a 2024 CDC Health Advisory flagged that medication shortages and major disruptions to provider access raise the risk for injury and overdose. Patients who cannot fill a prescription start looking sideways, and the nootropic-peptide corner of the internet has been ready with confident answers.
The clinical reality is more careful. More than half of individuals with ADHD, and significantly more women than men, were diagnosed in adulthood according to the CDC's 2024 MMWR data, the agency's first prevalence update in nearly 20 years. That late-diagnosis cohort, often functional but exhausted, is exactly the group asking whether something other than methylphenidate or lisdexamfetamine might help. Peptides keep surfacing in that search, and one name dominates.
Semax is the only peptide proposed as an ADHD candidate in print#
Semax is a synthetic heptapeptide. It is an analogue of the N-terminal fragment (4-10) of adrenocorticotropic hormone, but completely devoid of any hormonal activity, and has been found to stimulate memory and attention in rodents and humans after intranasal application; animal evidence has shown Semax can augment the effects of psychostimulants on central dopamine release and also stimulates central brain-derived neurotrophic factor (BDNF) synthesis.
A 2006 paper indexed on PubMed was the first to spell out the ADHD hypothesis explicitly. Psychostimulants such as methylphenidate are the most commonly used drug therapy for children with ADHD, but a number of patients either fail to respond or experience side effects that preclude their use.
The authors argued that because Semax could improve selective attention and modulate brain development, and because ADHD is likely a neurodevelopmental disorder with disturbance in dopamine and BDNF function, Semax may have therapeutic value worth investigating.
Note the verb tense. The paper proposed Semax as a candidate. It did not demonstrate efficacy in a randomised ADHD trial. Twenty years later, that gap has not been filled by a Western replication.
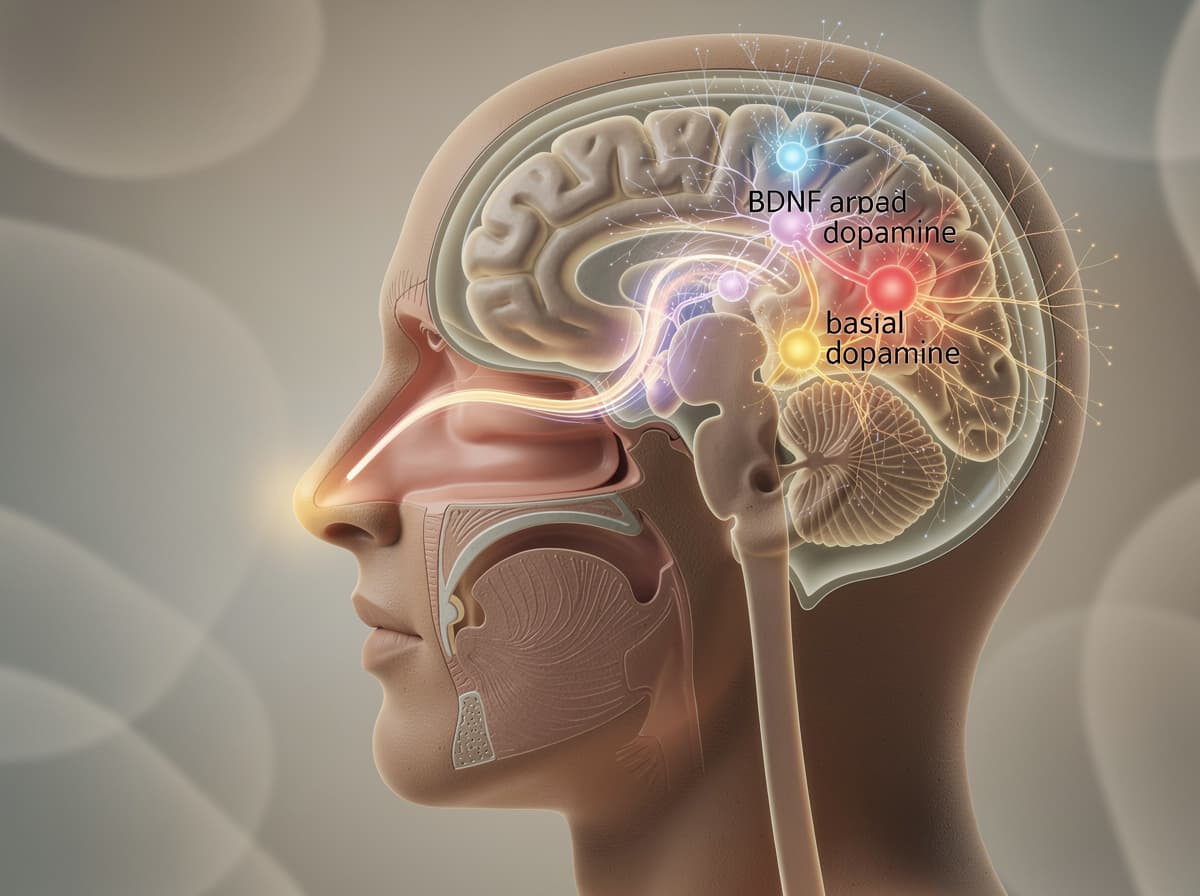
The BDNF mechanism is the most replicable part of the story#
If the clinical record is thin, the molecular record is unusually detailed for a peptide of this size. Sandwich immunoenzymatic analysis has shown that Semax applied intranasally at 50 and 250 micrograms per kilogram bodyweight produces a rapid increase in BDNF levels after three hours in the basal forebrain, but not in the cerebellum.
These findings, published in the Journal of Neurochemistry, point to specific binding sites for Semax in the rat basal forebrain and indicate that the cognitive effects exerted by Semax may be associated, at least in part, with increased BDNF protein levels in this brain region.
BDNF matters for the ADHD conversation because neurotrophins, including BDNF, are essential for neural growth, survival, and differentiation, and are therefore crucial for brain development, and ADHD is a neurodevelopmental disorder characterised by problems of inattention and/or hyperactivity-impulsivity. Whether modulating BDNF in adults durably shifts ADHD symptoms is a different question, and one the existing trials cannot answer.
The mechanism is also broader than BDNF alone. Semax upregulates BDNF and its receptor TrkB in the hippocampus and cortex, and also modulates expression of hundreds of genes involved in neuronal survival, synaptic plasticity, and neurotransmitter metabolism affecting serotonergic, dopaminergic, and cholinergic systems. That transcriptional breadth is what makes the peptide interesting and what makes it difficult to predict in an individual.
The regulatory split tells you what you need to know#
Semax has a clinical track record. It just is not a Western one. Semax is a synthetic heptapeptide analog of ACTH(4-10) developed in Russia in the 1980s as a neuroprotective and nootropic agent, is approved in Russia and on the Russian List of Vital & Essential Drugs for ischemic stroke recovery and cognitive impairment, and is not approved by FDA, EMA, or other Western regulators.
This asymmetry is the central honesty problem for anyone writing about peptides and ADHD. Russian neurology has decades of clinical use behind Semax, but most of that literature has not been replicated in large randomised Western trials, and individual ADHD pilot studies remain small. Treat any source that calls Semax a "proven ADHD solution" as marketing. The accurate framing: preliminary evidence is genuinely interesting, and the regulatory status reflects the absence of confirmatory trials.
Selank gets miscategorised as an attention peptide#
Selank often appears alongside Semax in "peptides for ADHD" listicles. The mechanism does not actually fit. Selank includes a short fragment (Thr-Lys-Pro-Arg) of the human immunoglobulin G heavy chain, elongated at the C-terminus via the addition of three natural L-amino acids (Pro-Gly-Pro) to enhance its metabolic stability and length of action. Its clinical record is anxiolytic, not pro-attentional.
A clinical comparison study found that in 62 patients with generalised anxiety disorder and neurasthenia, the anxiolytic effects of selank (30 patients) and medazepam (32 patients) were similar, but selank also had antiasthenic and psychostimulant effects. The "psychostimulant" descriptor in that paper is doing a lot of work for marketing copy that wants to call Selank an ADHD peptide. It refers to a mild activating effect in anxious-asthenic patients, not to dopaminergic stimulation of the kind seen with ADHD medications.
Where Selank may actually matter for an ADHD-adjacent patient is the comorbidity profile. According to a national 2022 parent survey, about 4 in 10 children with ADHD had anxiety. An anxiety load layered on attention dysregulation is common in adults too, and research suggests Selank's GABAergic modulation could support that adjacent domain, not the core inattention symptom cluster itself.
What the pilot ADHD data actually says, and what it does not#
The most-cited Semax ADHD pilot lives outside mainstream Western databases. Secondary summaries report that a pilot study in 45 children with ADHD found Semax treatment (intranasal administration, dose-adjusted for age and weight) improved attention span, reduced impulsivity, and enhanced academic performance as rated by parents and teachers using standardised ADHD rating scales, with effects comparable to conventional stimulant medications but a different side effect profile, notably lacking appetite suppression and sleep disturbances commonly associated with stimulants.
Read that carefully. It is a single pilot, n=45, in children, reported in Russian-language sources. Studies have shown the mechanism is plausible and the pilot signal is suggestive. None of that is the same as a confirmed effect in an adult Western ADHD population at a defined dose.
ClinicalTrials.gov does not currently list a registered randomised controlled trial of Semax for adult ADHD. Until that changes, the honest summary is: preliminary evidence points one direction, but the trial that would settle the question has not run.
How to think about peptides for ADHD without overclaiming#
Three principles keep the conversation honest.
First, mechanism is not outcome. BDNF upregulation in rat basal forebrain is real and replicated. After Semax administration, multidirectional activation of NGF and BDNF gene expression has been observed in the hippocampus, frontal cortex, and retina, with BDNF expression significantly increased 90 minutes after Semax administration in the retina. Translating that into "Semax fixes ADHD focus" skips every step that matters.
Second, the comparator question is unavoidable. Stimulant medications have a 60-year safety database and well-characterised response rates. Peptides do not. A patient whose stimulants work is not a candidate for peptide swapping; a patient whose stimulants fail, cause intolerable side effects, or are physically unobtainable is in a different conversation, and that conversation belongs in a clinic.
Third, the research-frame matters. Semax has been widely studied in Eastern European research contexts, particularly in neurology and cognitive science, and is typically positioned within a research-use framework. Klarovel's protocol layer is built for exactly that: structured logging, dose tracking via the peptide calculator, and partner sourcing where the regulatory status permits. It is not a substitute for psychiatric care.
The honest position on peptides for ADHD#
Semax has the most coherent mechanistic case of any peptide associated with attention, and the BDNF and dopamine pathways it touches are exactly the systems implicated in ADHD neurobiology. It also has a hypothesis paper, a small pilot in children, and a regulatory record that stops at the Russian border. That combination earns curiosity, not certainty.
Klarovel's view: track the protocol layer rigorously, source from verified partners where the law permits, and keep psychiatric care in psychiatric hands. If a peptide approach makes sense for an individual situation, it makes sense as a logged, measured research protocol, not as a stimulant substitute. Start with how it works, set up structured tracking, and register to begin a protocol with the visibility the science actually deserves.
Frequently asked questions
Keep reading

Peptides for Dementia: What the Clinical Evidence Actually Shows
A clinical look at Cerebrolysin, Semax, and Dihexa for dementia. Trial data, real limits, and why the peptide-dementia story needs honest framing.
Peptides for Focus: What the Cognitive Research Actually Shows
A clinical look at Semax, Selank, and Dihexa: how each peptide works on attention and focus, what studies report, and where the evidence still thins out.
Peptides for Anxiety: What the Research Actually Shows
A clinical-grade review of peptides studied for anxiety, including Selank, Semax, and oxytocin, with evidence, mechanisms, and realistic expectations.