
The choice between GH-secretagogue peptides and testosterone replacement therapy is rarely about which compound is "stronger." It is about which axis is actually broken. This comparison breaks down the mechanism, evidence, dosing reality, and side-effect profile of both, then gives a decision rule.
Key takeaways#
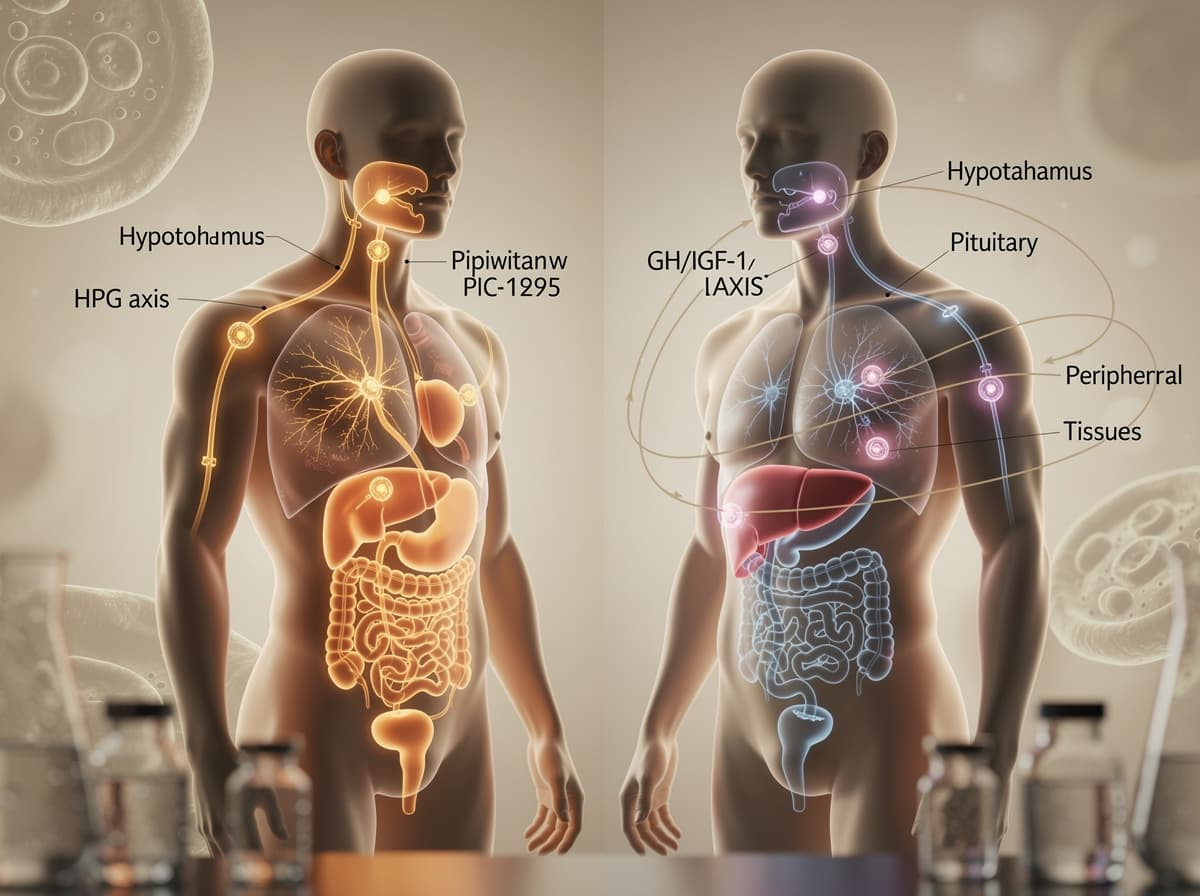
- Peptides like CJC-1295 and ipamorelin act on the GH/IGF-1 axis; TRT acts on the HPG (testosterone) axis. They are not interchangeable.
- TRT has decades of human outcome data including the 5,204-patient TRAVERSE cardiovascular trial; GH-secretagogue stacks have far smaller, mostly preclinical and early-phase human datasets.
- TRT typically suppresses endogenous testosterone production and fertility within months; GH secretagogues preserve pulsatile feedback and do not suppress the HPG axis.
- For diagnosed hypogonadism with symptoms, TRT is the standard of care. For body composition, recovery, and sleep quality in eugonadal adults, GH-secretagogue research is the more proportionate starting point.
- Stacking the two is biologically possible because the axes are independent, but it doubles monitoring complexity and is not a standard research protocol.
How peptides work in this comparison#
The "peptides" side of this match-up usually means GH secretagogues, most often a CJC-1295 plus ipamorelin pairing, sometimes tesamorelin. These compounds do not deliver growth hormone. They prompt the pituitary to release its own. CJC-1295 is a synthetic GHRH analogue that binds the GHRH receptor on anterior pituitary somatotrophs, activating Gs-protein signalling and cAMP-driven GH gene expression. Ipamorelin is a pentapeptide that hits a different target: the growth hormone secretagogue receptor type 1a, the ghrelin receptor on the same somatotroph cells, triggering calcium-dependent GH release.
The two pathways are independent, which is why the pair shows complementary action in mechanistic work. Co-administration of a GHRH analogue and a GHRP-class peptide has been shown to produce GH release 6 to 10 times greater than either peptide alone at matched doses. Crucially, ipamorelin is selective: at GH-effective research doses it produces minimal cortisol or prolactin co-stimulation, which is the main reason it displaced GHRP-2 and GHRP-6 in modern protocols. Tesamorelin is a separate animal: a stabilised GHRH analogue with FDA approval for HIV-associated lipodystrophy, giving it the most rigorous human safety dataset of any GH-secretagogue peptide.
The shared feature: these compounds preserve the natural pulsatile pattern of GH release and remain subject to negative feedback from IGF-1. They do not flatten the axis.
How TRT works in this comparison#
Testosterone replacement therapy substitutes exogenous testosterone for what the testes are no longer producing in adequate amounts. The target diagnosis is hypogonadism, and modern guidelines require two morning fasting testosterone levels below 300 ng/dL alongside symptoms before initiation. Routes include transdermal gels, intramuscular or subcutaneous injections of testosterone cypionate or enanthate, long-acting undecanoate injections, subcutaneous pellets, and oral undecanoate. Each route produces a different pharmacokinetic curve and a different side-effect emphasis.
Mechanistically, exogenous testosterone binds androgen receptors throughout the body and aromatises to estradiol at variable rates depending on body composition. The clinical effects, restored libido, improved erectile function, increased lean mass, reduced visceral fat, better mood, are well documented in hypogonadal men. The trade-off is that exogenous testosterone suppresses the hypothalamic-pituitary-gonadal axis. LH and FSH drop, intratesticular testosterone falls, and spermatogenesis is impaired in nearly all men on monotherapy TRT. This is the central biological difference from the peptide side.
Dosing: peptides vs TRT#
Research-published dose ranges differ in unit, frequency, and pharmacokinetic philosophy.
For the GH-secretagogue side, research protocols typically pair CJC-1295 (no-DAC) at roughly 100 mcg with ipamorelin at 100 to 300 mcg, administered subcutaneously once to three times daily, often timed pre-bed to align with the natural overnight GH pulse. Tesamorelin's FDA-approved dose for HIV-associated lipodystrophy is 1.28 mg subcutaneously once daily (per the current EGRIFTA WR label; the prior EGRIFTA SV product used 2 mg once daily). CJC-1295 with DAC sits outside this profile because its multi-day half-life flattens the pulse pattern.
For TRT, the TRAVERSE trial used daily transdermal 1.62% testosterone gel, dose-adjusted to maintain testosterone levels between 350 and 750 ng/dL. Injectable testosterone cypionate is commonly published in 100 to 200 mg per week, split into two doses to flatten peaks and troughs. Subcutaneous testosterone pellets are dosed at 150 mg to 450 mg every 3 to 6 months. Oral testosterone undecanoate (TLANDO) was studied at 225 mg twice daily with a meal.
The cadence difference matters. Peptide protocols demand near-daily compliance and timing discipline. TRT, especially pellets or long-acting injectables, can run on weekly or quarterly intervals. That practical asymmetry shapes adherence and lifestyle fit.
Evidence: what the studies actually show#
The evidence bases are not comparable in scale.
TRT has the TRAVERSE trial, a randomised, double-blind, placebo-controlled study of 5,204 hypogonadal men aged 45 to 80 with established or high-risk cardiovascular disease. Over a median follow-up of 33 months, testosterone therapy was non-inferior to placebo on the primary composite endpoint of cardiovascular death, non-fatal MI, and non-fatal stroke. In response, the FDA updated testosterone product labelling in February 2025, removing the Black Box language related to cardiovascular outcomes. Studies have shown clear improvements in sexual function, anemia, bone density, and body composition in hypogonadal men, though TRAVERSE did flag specific secondary signals worth taking seriously.
The peptide side is thinner. Tesamorelin's lipodystrophy trials are the strongest data point: studies have shown that tesamorelin reduces visceral adipose tissue by approximately 15 to 18% versus placebo over 26 weeks in HIV-associated lipodystrophy. For CJC-1295 and ipamorelin individually, preliminary evidence includes small healthy-adult pharmacokinetic studies showing sustained GH and IGF-1 elevation with CJC-1295 in healthy adults, and ipamorelin's selectivity profile is documented in early human pharmacology work. Research suggests the combination is mechanistically sound, but no large outcome trial of the CJC-1295 plus ipamorelin stack on body composition, sleep, or recovery in healthy adults exists.
This evidence gap is the most honest single fact in the peptides vs TRT comparison.

Side effects and contraindication profile#
The peptide side is associated with water retention, transient injection-site reactions, tingling or numbness from elevated GH or IGF-1, mild blood-glucose elevation (GH is counter-regulatory to insulin), and rare immunogenicity. Preclinical data points and FDA review documents named immunogenicity as a flagged signal for ipamorelin and CJC-1295. The most important hard contraindication is active or recent malignancy, because GH and IGF-1 promote cell proliferation. Insulin resistance and pre-diabetes warrant tighter glucose monitoring.
TRT's signature risks are well-characterised. Erythrocytosis (rising hematocrit) is the most common dose-related adverse effect and requires periodic monitoring. The TRAVERSE results, while reassuring on the primary endpoint, flagged an increased risk of non-fatal arrhythmias, venous thromboembolic events, and fractures in the testosterone group compared to placebo. Atrial fibrillation showed up as a specific concern. Suppression of spermatogenesis is the near-universal outcome for any man on monotherapy TRT; men wanting fertility within 12 months typically pair TRT with hCG or avoid TRT entirely in favour of clomiphene or enclomiphene. Prostate monitoring is standard, and current Endocrine Society guidance recommends urological consultation if PSA rises during the first 12 months.
Overlap zone: both can affect glucose handling and both demand baseline plus follow-up bloodwork. Divergence zone: only TRT suppresses the HPG axis, and only TRT carries the documented hematocrit and VTE signals at clinically relevant frequencies.
When to choose peptides#
Choose the GH-secretagogue route when:
- Bloodwork shows testosterone in the normal range but body composition, sleep depth, or recovery are the actual complaints.
- Fertility preservation is a hard requirement in the next 12 to 24 months.
- The goal is research-context exploration of GH-axis effects rather than substitution for a deficient hormone.
- Visceral adiposity is the dominant issue and tesamorelin's specific profile maps to the complaint (its strongest evidence is preliminary evidence from HIV-associated lipodystrophy, but the mechanistic logic extends to general visceral fat reduction in research settings).
When to choose TRT#
Choose testosterone replacement when:
- Two morning fasting testosterone readings are below 300 ng/dL (or 10.4 nmol/L) and symptoms of hypogonadism are present, low libido, erectile dysfunction, fatigue, mood changes, loss of lean mass.
- Hypogonadism is confirmed and fertility is not a near-term goal, or fertility-preserving co-therapy is on the table.
- The bone density, anemia, or sexual function dimensions are dominant; these are the domains where TRT has been shown to produce reliable, replicable effects.
- The patient profile matches the TRAVERSE inclusion criteria (middle-aged or older with documented hypogonadism), because that is where the cardiovascular safety data is strongest.
Can you stack peptides and TRT?#
Mechanistically, yes. The GH/IGF-1 and HPG axes are independent endocrine systems and the receptor targets do not overlap. In practice, stacking is uncommon in research literature because it compounds monitoring complexity: hematocrit, PSA, estradiol, IGF-1, fasting glucose, and lipid panels all become moving targets simultaneously. There is no head-to-head trial of TRT plus GH-secretagogue versus TRT alone in healthy or hypogonadal adults. Stacking is not standard practice because the marginal benefit is undocumented while the monitoring burden roughly doubles.
Verdict#
For confirmed hypogonadism with symptoms, TRT is the better starting point. It has a 5,204-patient cardiovascular safety trial behind it, a defined diagnostic threshold, and decades of body-composition and sexual-function data. The peptide side cannot match that evidence base in 2026.
For eugonadal adults whose complaint is sleep quality, recovery, body composition, or visceral fat (and whose testosterone is genuinely in range), a CJC-1295 plus ipamorelin protocol, or tesamorelin where visceral fat is dominant, is the more proportionate intervention. Pushing testosterone above the physiological range to chase those same outcomes is the wrong tool. The decisive variable is the bloodwork, not the marketing.
Make the comparison personal, not generic#
Peptides vs TRT is the wrong question phrased at the right altitude. The right question is which axis your bloodwork actually flags, and which intervention has the evidence base to match the complaint. Quantify your own numbers with the peptide calculator, work through the Klarovel questionnaire to translate symptoms into a research direction, and read how Klarovel curates protocols before deciding which side of this comparison maps to you.
Frequently asked questions
Keep reading

MK-677 vs Tesofensine: GH Support vs Fat Loss (2026)
MK-677 raises GH and appetite; tesofensine is a central appetite suppressor with 9% weight loss. Head-to-head on mechanism, dose, and evidence.
KPV vs Thymosin Alpha-1: Which Wins for Gut and Immune?
KPV calms inflammation in the gut and skin. Thymosin alpha-1 modulates immunity. A head-to-head on mechanism, evidence, and when to pick which.
Ipamorelin vs Hexarelin: Clean Signal or Raw Potency (2026)
Ipamorelin vs hexarelin, compared on GH pulse size, cortisol impact, cardiac effects, and desensitization. Which GHRP actually fits your protocol.