Two molecules dominate every fat-loss search in 2026, and they could not be more different. AOD-9604 is a synthetic fragment of growth hormone marketed as a "targeted" lipolytic; semaglutide is a GLP-1 analogue with the largest obesity trial portfolio of any pharmacological agent in history. The honest comparison is not even close on efficacy, but the mechanism contrast is real, and choosing between them depends on what the reader actually needs.
Key takeaways#
- Semaglutide produces roughly 5-6x the placebo-adjusted weight loss of AOD-9604 in head-to-head trial comparisons across published Phase 2/3 data.
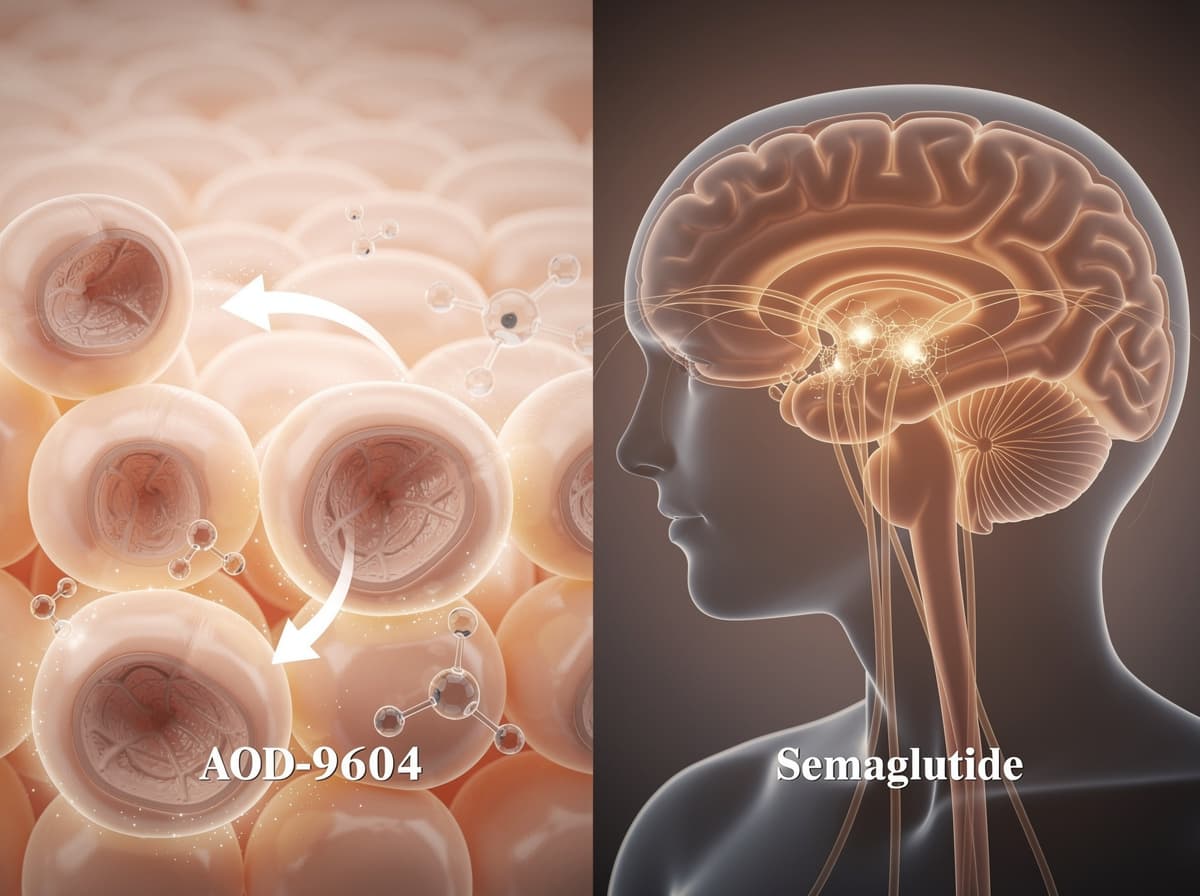
- AOD-9604 acts peripherally on adipocytes to stimulate lipolysis; semaglutide acts centrally on hypothalamic GLP-1 receptors to reduce energy intake.
- In the STEP 1 trial, semaglutide 2.4 mg weekly produced a mean weight change of -14.9% at week 68 vs -2.4% with placebo across 1,961 adults.
- AOD-9604's Phase 2b program failed its primary endpoint and development was terminated in 2007; the molecule has no major-regulator approval for any indication.
- Stacking is mechanistically plausible but unstudied in controlled trials; the side-effect profiles do not overlap, which is the only honest case for the combination.
How AOD-9604 works#
AOD-9604 is a 16-amino-acid analogue of the C-terminal fragment of human growth hormone (residues 177-191) with a tyrosine added at the N-terminus. It is an orally active analogue of a peptide fragment of human growth hormone that selectively activates lipolysis in adipose tissue. The mechanism is peripheral, not central: the fragment binds adipocyte receptors and triggers cAMP-mediated hormone-sensitive lipase activity, releasing free fatty acids and glycerol from stored triglycerides. Critically, AOD-9604 was engineered to leave growth hormone receptor signalling alone, which is why it does not raise IGF-1 or impair glucose tolerance the way full-length GH does.
Research has shown the lipolytic signal is real but isolated. A controlled human pharmacodynamic study confirmed that subcutaneous AOD-9604 increased plasma glycerol and free fatty acids, the textbook biomarkers of triglyceride breakdown. The clinical problem is what happens next. Liberated fatty acids must be oxidised in muscle or liver mitochondria; if energy expenditure is not elevated and intake is not constrained, the fatty acids re-esterify back into triglycerides. Lipolysis without an oxidation sink does not equal net fat loss, and that is the gap the human trials fell into.
How semaglutide works#
Semaglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist. It induces weight loss by decreasing appetite, thereby improving control of eating and reducing energy intake. The drug is a long-acting GLP-1 analogue engineered for a half-life of roughly a week, which allows once-weekly subcutaneous dosing. The action is dominantly central: GLP-1 receptors in the hypothalamus and hindbrain modulate satiety, slow gastric emptying, and reduce reward-driven eating. Glucose-dependent insulin secretion is a secondary effect that matters more for diabetes indications than for obesity outcomes.
Studies have shown that the satiety mechanism produces a large, sustained reduction in caloric intake without the metabolic compensation that defeats most diet interventions. That is the load-bearing distinction. AOD-9604 makes fat available for oxidation; semaglutide reduces what enters the system in the first place. The two molecules are not interchangeable tools for the same job.
Dosing: AOD-9604 vs semaglutide#
For AOD-9604, the Phase 2b clinical programme tested oral doses up to 1 mg daily over 24-week treatment windows. Subcutaneous research protocols typically range from 250 to 500 mcg per day, often administered fasted in the morning to avoid insulin opposition of the lipolytic signal. There is no FDA-approved dose because the molecule was never approved.
For semaglutide, the Wegovy label specifies a titration to 2.4 mg once weekly subcutaneously for chronic weight management, with a starting dose of 0.25 mg weekly and stepwise increases over 16-20 weeks to manage GI tolerability. Ozempic for type 2 diabetes runs lower (0.5-2.0 mg weekly). Self-titration off-label is the single most common mistake in semaglutide protocols; the escalation schedule exists because nausea and vomiting scale steeply with the jump.
Evidence: what the studies actually show#
Semaglutide (STEP 1): the pivotal 68-week, double-blind trial randomised 1,961 adults with BMI ≥30 (or ≥27 with a coexisting condition) to 2.4 mg weekly semaglutide or placebo, both with lifestyle intervention. Results have been shown to be robust: the estimated mean weight change at week 68 was -14.9% with semaglutide vs -2.4% with placebo, a 12.4 percentage-point treatment difference (95% CI -13.4 to -11.5; P<0.001). Cardiovascular outcomes in the SELECT trial extended that signal, showing semaglutide reduced major adverse cardiovascular events in adults with overweight or obesity and preexisting cardiovascular disease but no diabetes.
AOD-9604 (OPTIONS / METAOD006): the largest controlled study, a 24-week Phase IIb trial with roughly 500 obese subjects randomised to oral AOD-9604 at doses up to 1 mg daily or placebo, failed to meet its primary efficacy endpoint. An earlier shorter trial had shown a modest signal, but that effect did not scale or sustain at the larger sample size. Independent fact-check synthesis of the program concludes that AOD-9604 has robust preclinical lipolytic rationale and repeated human safety signals but lacks conclusive Phase 2 efficacy data demonstrating meaningful weight loss in humans; Metabolic Pharmaceuticals discontinued development in 2007. No major regulator has approved AOD-9604 for any indication since.
The asymmetry is not subtle. Semaglutide has multiple positive Phase 3 trials with effect sizes in the double-digit percentage points. AOD-9604 has preliminary evidence of pharmacodynamic activity, no positive Phase 2b primary endpoint, and a discontinued development program. Anyone framing them as "alternatives" is overstating the evidence base on the AOD-9604 side.
Side effects, contraindications, and selection#
The side-effect profiles barely overlap, which is the most interesting practical fact about this comparison.
Semaglutide's adverse-event profile is dominated by gastrointestinal symptoms. The STEP 1 conclusion was that 2.4 mg semaglutide weekly plus lifestyle intervention was associated with sustained, clinically relevant reduction in body weight, but that benefit comes with nausea, vomiting, diarrhoea, and constipation as the most common reasons for dose interruption. Pancreatitis, gallbladder events, and a boxed warning about thyroid C-cell tumours (extrapolated from rodent data) are the serious-event flags. Semaglutide is contraindicated in personal or family history of medullary thyroid carcinoma and MEN2.
AOD-9604's profile is, by all available accounts, mild. Phase 2 trials reported good tolerability and no meaningful changes in IGF-1 or glucose tolerance. The safety reassurance is real; the efficacy reassurance is not. There is no recognised contraindication list because there is no regulatory label, which is itself a flag, not a feature.
Preliminary evidence and Phase 2b human data together produce a clean decision rule. Choose semaglutide when the user has clinically meaningful weight to lose (BMI ≥27 with comorbidity or ≥30), tolerates GI side effects during titration, and wants the evidence-base. Choose AOD-9604 only in the narrow case of a research context targeting visceral or "stubborn" subcutaneous fat in someone already lean, in an energy deficit, training consistently, and not seeking double-digit weight loss. The catalog research-protocol dose range applies; nothing here is medical advice.

Can you stack them?#
Mechanistically, yes. AOD-9604 acts peripherally on adipocytes; semaglutide acts centrally on appetite. The pathways do not collide, and the side-effect profiles do not overlap. Combined, you would in theory get caloric restriction from semaglutide plus enhanced fatty-acid availability from AOD-9604, which is the textbook condition for net fat oxidation.
In practice, this combination has not been studied in any controlled trial. The community protocols stacking AOD-9604 with GLP-1 agonists are extrapolations from mechanism, not evidence. The honest framing: the stack is plausible, low-risk on paper, and unvalidated. If the goal is fat loss and the user already tolerates semaglutide at therapeutic dose, the marginal benefit of adding AOD-9604 is likely small relative to the trial-grade effect semaglutide is already producing.
Verdict#
For nearly every reader asking the question, semaglutide is the better starting point. The trial data are an order of magnitude stronger, the regulatory approval covers chronic weight management, and the cardiovascular outcomes signal in SELECT extends the case beyond pounds on a scale. AOD-9604 is interesting biology with a real but isolated pharmacodynamic effect, and a failed Phase 2b that nobody in the peptide marketing layer wants to discuss. It is a niche tool for a research context, not a viable alternative to a GLP-1 agonist for weight loss. If GLP-1 access is not an option or the side-effect profile is intolerable, AOD-9604 is a weak substitute, not an equivalent one. The Klarovel peptide calculator and intake questionnaire can map either compound onto the user's actual bloodwork and goals.
The honest comparison the rest of the internet won't make#
Klarovel's editorial position on this comparison is unusually clean: the evidence asymmetry is too large to soft-pedal. Semaglutide has the trial portfolio. AOD-9604 has interesting biology and a discontinued development program. Pick the tool that matches the goal, not the one that matches the marketing. For the wider field, see how the GLP-1 weight-loss medications compared stack up against one another. Quantify the choice against your actual bloodwork with the peptide calculator, see how Klarovel structures protocol guidance, and register to get the personalised framing the generic comparison content can't produce.
Frequently asked questions
Keep reading
Ipamorelin vs Hexarelin: Clean Signal or Raw Potency (2026)
Ipamorelin vs hexarelin, compared on GH pulse size, cortisol impact, cardiac effects, and desensitization. Which GHRP actually fits your protocol.

TB-500 vs Thymosin Beta-4: Fragment or Full-Length in 2026
TB-500 is a 7-amino acid fragment of thymosin beta-4's actin-binding site. Which one actually has human trial data? A head-to-head breakdown.

MK-677 vs tesamorelin: oral GH versus visceral fat (2026)
Head-to-head on MK-677 vs tesamorelin: oral ghrelin mimetic versus injectable GHRH analogue, with VAT data, glucose risk, and a clear decision rule.