Cagrilintide and semaglutide get framed as competitors, but the most interesting data of 2025 shows they are most powerful when paired. The REDEFINE trials reframed this entire comparison: the question is no longer "which one wins" but "when does each one make sense on its own, and when do you stack them?" This guide walks through the mechanism, the dosing, the trial data, and a clear decision rule.
Key takeaways#
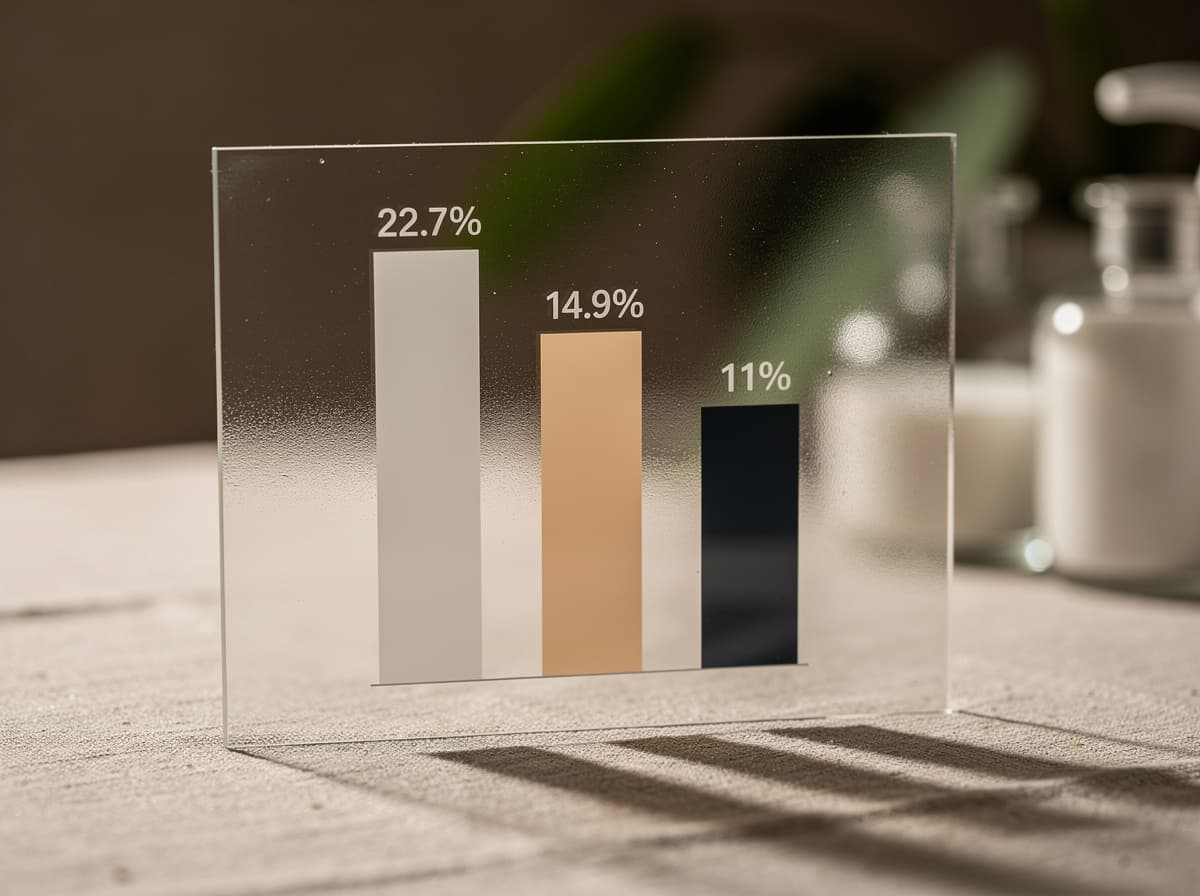
- Semaglutide is a GLP-1 receptor agonist with the largest single-agent obesity dataset in the world; STEP 1 documented a mean 14.9% weight reduction at 68 weeks.
- Cagrilintide is a long-acting amylin and calcitonin receptor agonist; as monotherapy at 2.4 mg it produces roughly 8 to 11% weight loss over 26 to 68 weeks.
- The combination (CagriSema) delivered 22.7% mean weight loss in REDEFINE 1, with 60% of participants losing 20% or more.
- Semaglutide has dedicated cardiovascular outcome data (a 20% MACE reduction in SELECT); cagrilintide does not yet have an equivalent CV endpoint trial.
- GI side effects are the dominant tolerability issue for both, and the combination roughly doubles the GI event rate compared to either agent alone.
How cagrilintide works#
Cagrilintide is a long-acting synthetic analogue of amylin, a 37-amino-acid hormone co-secreted with insulin from pancreatic beta cells. It binds amylin receptors (AMY1R, AMY2R, AMY3R) and the calcitonin receptor, putting it in the dual amylin and calcitonin receptor agonist (DACRA) class. In clinical trials, the half-life of cagrilintide (0.16 to 4.5 mg) ranged from 159 to 195 hours, with an elimination half-life of 7 to 8 days, making it suitable for once-weekly dosing.
The mechanism is non-incretin. Amylin slows gastric emptying in the stomach, suppresses post-prandial glucagon release in the pancreas, and activates homeostatic and reward centers in the brain to suppress appetite and reduce food intake. Critically, cagrilintide was engineered to prevent the amyloid-fibril aggregation that limits native amylin, using 14E and 17R mutations to create a stabilising salt bridge in the central helix. An N-terminal C20 fatty acid drives albumin binding and the long half-life.
Because the amylin and GLP-1 pathways are mechanistically independent, the rationale for combining cagrilintide with semaglutide is biological, not just additive. Research suggests the two molecules act on complementary brain regions involved in both hedonic and homeostatic appetite regulation.
How semaglutide works#
Semaglutide is a GLP-1 receptor agonist with a half-life of roughly 7 days, also suitable for once-weekly subcutaneous administration. It is the most extensively studied anti-obesity peptide on the market, with established weight-loss and cardiovascular indications under the Wegovy brand at the 2.4 mg dose. The mechanism is incretin-based: GLP-1 receptor activation increases glucose-dependent insulin secretion, suppresses glucagon when glucose is elevated, slows gastric emptying, and reduces appetite via hypothalamic and hindbrain signalling.
The pivotal weight-loss evidence comes from STEP 1. In adults with obesity or overweight with one or more weight-related coexisting conditions and without diabetes, mean weight loss was 14.9% from baseline with semaglutide as an adjunct to lifestyle intervention, exceeding placebo by 12.4 percentage points.
86% of participants attained at least 5% weight loss. The trial is published in NEJM.
The cardiovascular dataset is what sets semaglutide apart from every other obesity peptide. In the SELECT trial, once-weekly semaglutide compared with placebo produced a 20% reduction in major adverse cardiovascular events in individuals with overweight or obesity without diabetes. Full results are in JACC.
Dosing: cagrilintide vs semaglutide#
Both peptides use a slow titration schedule to manage GI tolerability. Research protocols typically share a similar cadence:
For semaglutide 2.4 mg (weight-management dose), research-published titration starts at 0.25 mg weekly, escalates every four weeks through 0.5, 1.0, 1.7 mg, and reaches the 2.4 mg maintenance dose by week 17.
For cagrilintide monotherapy, the phase 2 dose-finding protocol used the same step pattern: 0.25 mg, then 0.5, 1.0, 1.7, and 2.4 mg, with each dose held for four weeks before escalation. From a baseline weight of approximately 100 kg, treatment with 2.4 mg and 4.5 mg cagrilintide resulted in weight loss of 9.7% and 10.8% respectively at week 26, compared to 3.0% with placebo.
For CagriSema, the published phase 3 protocol escalates both molecules in parallel, ending at cagrilintide 2.4 mg plus semaglutide 2.4 mg once weekly. The slower the titration, the better the GI tolerability profile. Klarovel's peptide titration calculator generates the week-by-week escalation table for the semaglutide and cagrilintide arms so users can compare side-effect ramps against the actual dose schedule.
Evidence: what the studies actually show#
The two cleanest head-to-head datasets come from the REDEFINE program, which compared CagriSema to each monotherapy and to placebo.
REDEFINE 1 randomised 3,417 adults with overweight or obesity (without diabetes) in a 21:3:3:7 ratio to CagriSema, semaglutide 2.4 mg alone, cagrilintide 2.4 mg alone, or placebo over 68 weeks. CagriSema participants achieved a mean body weight reduction of 20.4%, compared to 3.0% with placebo at week 68, a treatment difference of 17.3 percentage points.
60% of participants receiving CagriSema achieved at least 20% weight loss, and 23% lost 30% or more. Cagrilintide alone in the same trial produced roughly 11.8% weight loss; semaglutide alone produced figures consistent with prior STEP data. Full results are in NEJM.
REDEFINE 2 enrolled adults with type 2 diabetes, a population that historically responds less to weight-loss pharmacotherapy. CagriSema achieved 13.7% weight loss compared to 3.4% with placebo. The combination also improved glycaemic control with a low incidence of hypoglycaemia.
For semaglutide as a standalone agent, the case is built on two pillars. STEP 1 documents the 14.9% mean weight reduction at 68 weeks. SELECT documents a 20% MACE reduction in patients with established cardiovascular disease but without diabetes, an outcome cagrilintide has not yet demonstrated independently. Preliminary evidence on CagriSema's cardiovascular profile is encouraging, with post-hoc analyses showing a 10.9 mmHg systolic blood pressure reduction in REDEFINE 1, but the dedicated CV outcomes trial (REDEFINE 3) is still ongoing.
Side effects and contraindication profile#
Both peptides carry the gastrointestinal signature of the appetite-suppression class. The key difference is magnitude when combined.
For semaglutide 2.4 mg monotherapy, the dominant adverse events are nausea (around 25% incidence), constipation, diarrhoea, and vomiting. Studies have shown most events are mild to moderate and concentrate during the dose-escalation window.
For cagrilintide monotherapy, the profile is similar but slightly different in distribution. Nausea is dose-dependent, with phase 2 data showing rates from roughly 20% at low doses to nearly 47% at 4.5 mg. Injection-site reactions are more common with cagrilintide than with semaglutide, an effect associated with the lipid-modified amylin structure.
For CagriSema, the combination amplifies the GI burden. Gastrointestinal adverse events affected 79.6% of the cagrilintide-semaglutide group versus 39.9% in the placebo group, including nausea, vomiting, diarrhoea, constipation, or abdominal pain, mainly transient and mild-to-moderate in severity.
Specifically, nausea was reported in 55% versus 12.6%, constipation in 30.7% versus 11.6%, and vomiting in 26.1% versus 4.1%. Despite that burden, discontinuation rates due to adverse events were low at 6% for CagriSema versus 3.7% for placebo.
Shared class-level contraindications: personal or family history of medullary thyroid carcinoma, multiple endocrine neoplasia syndrome type 2, and prior episodes of pancreatitis. Slowed gastric emptying can also affect the absorption of oral medications with narrow therapeutic windows.
When to choose cagrilintide#
Cagrilintide as a standalone protocol makes sense in a specific set of scenarios:
- The reader has tried a GLP-1 agonist and developed clinically meaningful intolerance, particularly persistent nausea that did not resolve through titration. Cagrilintide's amylin mechanism may support appetite regulation without re-triggering GLP-1-specific adverse events.
- The reader is interested in a non-incretin approach for mechanistic reasons (for instance, post-bariatric surgery contexts where GLP-1 axis manipulation is less desirable).
- The reader plateaued on GLP-1 monotherapy and wants to add a complementary mechanism rather than escalate semaglutide further. Preliminary evidence and the phase 1B data suggest cagrilintide can produce an additional 7.4% weight loss on top of semaglutide.
Cagrilintide as monotherapy is the weaker option when the primary outcome is maximum weight loss; semaglutide outperforms it head-to-head at standard doses.
When to choose semaglutide#
Semaglutide as a standalone protocol is the better starting point when:
- The reader's risk profile includes established cardiovascular disease. The SELECT data on a 20% MACE reduction is the strongest CV signal in the class.
- The reader has type 2 diabetes and needs glycaemic benefit alongside weight loss. Semaglutide has been shown to improve HbA1c independently of weight effects.
- Access and regulatory certainty matter. Semaglutide 2.4 mg is approved in the US and EU under the Wegovy brand; cagrilintide is still unapproved.
- The reader is treatment-naive and wants the most studied, most predictable starting point in the obesity-peptide category.
Can you stack them?#
Yes, and the stack is the most evidence-backed combination protocol in obesity pharmacology as of 2026. CagriSema is a fixed-dose combination of cagrilintide 2.4 mg and semaglutide 2.4 mg, designed for once-weekly subcutaneous administration. Studies have shown the two molecules hit complementary receptor families and produce supra-additive weight loss compared to either alone.
The trade-off is tolerability. The combination roughly doubles the GI event rate. For most readers, the practical sequence is: establish tolerance on semaglutide first, reach maintenance dose, then evaluate whether the additional 5 to 8 percentage points of weight loss from adding cagrilintide is worth the additional GI burden. Stacking from day one is not standard practice outside of the REDEFINE protocol design.
Verdict#
For most adults with overweight or obesity and no specific contraindication, semaglutide is the better single-agent starting point. It has the larger evidence base, the dedicated cardiovascular outcome data, and the regulatory approval. Cagrilintide monotherapy underperforms semaglutide on weight loss in head-to-head data and lacks an equivalent CV trial.
But the framing as a binary choice misses the point. Research has shown the combination is where the real ceiling lives: a mean 22.7% weight reduction with 60% of participants losing at least 20% is the highest range of any non-surgical intervention. If the goal is maximum weight loss and the reader can tolerate the GI side effects, the CagriSema-style stack is the protocol the evidence points to. If the goal is the strongest cardiovascular signal, semaglutide alone remains the cleaner choice until REDEFINE 3 reads out.
The decision rule, in one sentence#
If the priority is cardiovascular risk reduction and regulatory certainty, semaglutide is the answer; if the priority is maximum weight loss and the reader can tolerate the GI burden, the CagriSema-style stack is where the evidence points. To quantify which one a specific bloodwork and goal profile actually favours, run the inputs through the peptide calculator and start with the questionnaire, then cross-reference against the cagrilintide complete guide, the wider overview of how the GLP-1 weight-loss medications compared, and the disclosures at /disclosures before committing to a protocol direction.
Frequently asked questions
Keep reading

MK-677 vs Tesofensine: GH Support vs Fat Loss (2026)
MK-677 raises GH and appetite; tesofensine is a central appetite suppressor with 9% weight loss. Head-to-head on mechanism, dose, and evidence.
KPV vs Thymosin Alpha-1: Which Wins for Gut and Immune?
KPV calms inflammation in the gut and skin. Thymosin alpha-1 modulates immunity. A head-to-head on mechanism, evidence, and when to pick which.
Ipamorelin vs Hexarelin: Clean Signal or Raw Potency (2026)
Ipamorelin vs hexarelin, compared on GH pulse size, cortisol impact, cardiac effects, and desensitization. Which GHRP actually fits your protocol.