Delta sleep-inducing peptide has circulated in biohacker forums for years as the quiet alternative to GABAergic sedatives. The actual literature is older, smaller, and more ambivalent than the marketing suggests. This guide separates what the primary research has shown from what the supplement-adjacent internet has invented.
Key takeaways#
- DSIP is a nine-amino-acid neuropeptide first isolated in 1977 from the cerebral venous blood of rabbits in induced sleep, with the sequence Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu.
- The seminal 1978 human trial used 25 nmoles/kg intravenously in six chronic insomniacs and reported longer sleep duration with no daytime sedation.
- Animal work shows clean increases in slow-wave sleep, but later human plasma studies found DSIP levels are actually highest in the afternoon and lowest at night, complicating the "endogenous sleep factor" story.
- The U.S. FDA lists DSIP among bulk drug substances flagged for significant safety risks, citing potential immunogenicity in compounded formulations.
- Klarovel does not sell DSIP. Research-grade material is available from specialised suppliers and any structured trial belongs inside a documented protocol, not casual self-experimentation.
DSIP is a nonapeptide, not a sedative#
DSIP is a small, naturally occurring nonapeptide. A peptide which induces slow-wave EEG sleep after intraventricular infusion into the brain was isolated from the extracorporeal dialysate of cerebral venous blood in rabbits submitted to hypnogenic electrical stimulation of the intralaminar thalamic area, shown by amino-acid analysis to be Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu and named "Delta Sleep-Inducing Peptide" (DSIP) . That is the entire molecule: nine residues, molecular weight around 850 daltons, amphiphilic enough to cross membranes more readily than most peptides its size.
What matters mechanistically is what DSIP is not. It is not a benzodiazepine, not a Z-drug, not an antihistamine. DSIP has been described as a sleep-promoting substance rather than a sedative. There is a modulating effect on sleep and wake functions with a greater activity in circumstances where sleep is disturbed. There are minimal effects in healthy subjects who are not suffering from sleep disturbance. That distinction matters: a sedative knocks down a healthy brain, while DSIP appears to normalise a dysregulated one, or fail to do much at all. The implication is that anyone with already-decent sleep is unlikely to notice anything.
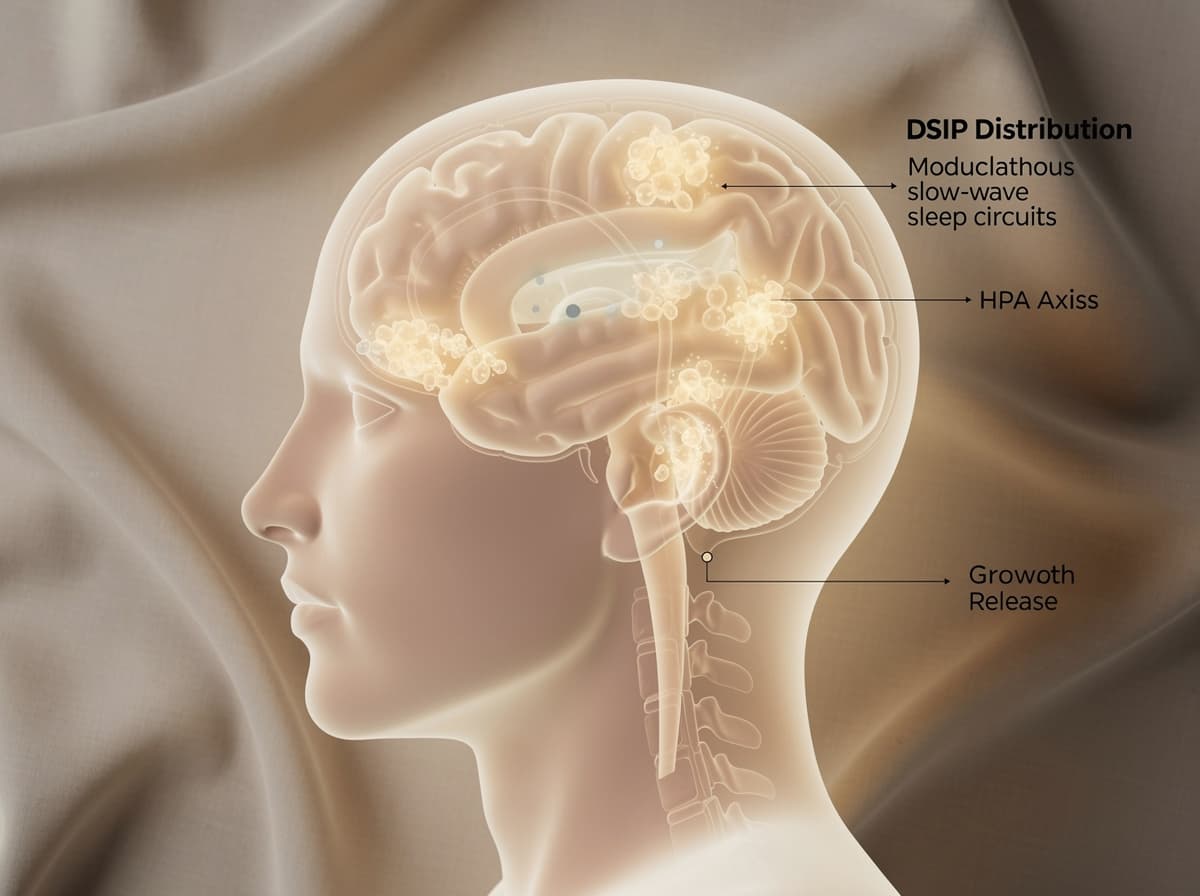
Distribution is broad. The peptide has been mapped in the hypothalamus, limbic system, and pituitary, and DSIP-like immunoreactivity has been measured in human breast milk and plasma. That endogenous footprint is what originally drove the "natural sleep factor" hypothesis, although as discussed below the diurnal data complicate the picture.
The 1978 human trial is still the cleanest data point#
Despite half a century of interest, the published human evidence remains thin. The most-cited study is a small Schoenenberger-Monnier group trial from the late 1970s. The effects of acute intravenous administration of synthetic DSIP at 25 nmoles/kg body weight on disturbed human sleep were tested in six middle-aged chronic insomniacs. The results were longer sleep duration and higher quality sleep with fewer interruptions, slightly more REM sleep, but no daytime sedation or other side effects, though the sleep-enhancing capacity was seen for up to six hours of night sleep. Sleep-promoting effects occurred only in the second hour after injection; in the first hour a slight arousing effect was indicated. That "first-hour arousal" is rarely mentioned in modern marketing and is one of several reasons casual subcutaneous dosing right before bed may not replicate the IV-trial timing.
Research suggests effective doses in published human work cluster around 25 nmoles/kg intravenously, which for a 75 kg adult is roughly 1.6 mg total per session. That is substantially higher than what circulates in self-experimentation forums, where subcutaneous doses of 100-300 mcg before bed are common. Pharmacokinetics differ between routes, and the gap between the clinical literature and forum practice is wider than most users realise.
The broader review picture, summarised in a 2001 editorial in the European Journal of Anaesthesiology, is that DSIP studies have produced "varied success" and that the effect is strongest in subjects with disturbed sleep rather than healthy controls.
Animal data are cleaner than human data#
Where the human signal is modest, the animal signal is more consistent. In a cat study, a single intracerebroventricular injection of synthetic DSIP at 7 nmol/kg produced a significant decrease in sleep latency, an increase in total sleep, and a selective increase in deep slow-wave sleep (S2), while REM architecture was unaffected. DSIP was immediately effective since the amount of S2 increased to more than 50% in the first postinjection hour and the difference from the control value was highly significant.
A phosphorylated analogue extended the effect further. Continued 10-h nocturnal intracerebroventricular infusion of 0.5 nmol P-DSIP, the phosphorylated analogue of delta-sleep-inducing peptide, significantly increased slow wave sleep (22%) and paradoxical sleep (81%) in unrestrained rats.
Larger and smaller doses were ineffective in doses ranging from 0.025 to 25 nmol. The sleep-promoting potency of P-DSIP was 5 times greater than that of DSIP compared by the same assay. The dose-response curve is sharply non-linear, which is a recurring theme in peptide research and a strong argument against the "more is better" assumption.
Preclinical data points also tie DSIP to growth hormone release during slow-wave sleep. In a rodent passive-immunisation study, sleep deprivation caused a significant increase in GH release and in the amount of slow-wave sleep above initial values, and these increases were blocked by microinjection of highly specific antiserum to DSIP . That suggests DSIP is not just correlated with deep sleep but functionally upstream of one of its hormonal signatures.
The diurnal-rhythm paradox#
Here is where the simple "DSIP equals sleep" story breaks. When researchers measured circulating DSIP across 24 hours in healthy humans, the rhythm ran opposite to what an endogenous sleep factor should look like. There was a distinct diurnal rhythm for plasma DSIP levels, with the maximum at 1500 h and the minimum at 0100 h. DSIP levels were substantially lower in REM sleep and somewhat lower in slow-wave sleep compared to awake values, and did not rise before, during, or after a significant percentage of episodes of slow-wave sleep. The diurnal rhythm closely followed that of body temperature with a high degree of correlation.
The investigators concluded that endogenous elevations of circulating DSIP may be associated with suppression of slow wave and rapid eye movement sleep, and that the circadian rhythm of this peptide is coupled directly or indirectly to that of body temperature . A follow-up study confirmed that plasma DSIP drops at the transition from wakefulness to sleep, reinforcing the paradox.
There are several possible reconciliations: peripheral plasma DSIP may not reflect central CNS pools; exogenous administration may engage receptors that endogenous fluctuations do not; or the "sleep-promoting" effect of DSIP is really a thermoregulatory or HPA-axis effect that secondarily improves sleep continuity. The honest position is that the mechanism remains unresolved, which is why a 2006 review titled DSIP a "still unresolved riddle" almost two decades ago, and the riddle has not been solved since.
Safety profile and the FDA's current stance#
The older European literature characterises DSIP as remarkably well tolerated. No significant side-effects have so far been reported with DSIP. In some human studies, transient headache, nausea and vertigo have been reported. DSIP actually appears to be incredibly safe as its LD50 has never been determined. That tolerability is a real finding from decades of small studies, but it is not the whole regulatory picture.
The current U.S. position is more cautious. The FDA has included DSIP on its list of bulk drug substances with significant safety risks. Per the FDA, compounded drugs that contain DSIP may pose a risk for immunogenicity, a state in which the body perceives a substance as a threat and mounts a potentially life-threatening immune response against it. Norwegian and EU regulators have not issued DSIP-specific guidance, but Legemiddelverket's general framework around unlicensed compounded peptides applies: import for personal use sits in a grey zone, and any research-grade material should be handled accordingly.
The practical implication is that the "incredibly safe" framing from 2001 reflects acute exposure in supervised trials. Long-term safety, batch-to-batch immunogenicity, and the consequences of repeated subcutaneous dosing are not characterised. Safety and possible side-effects of long-term DSIP use haven't been established in clinical research studies.
Where DSIP fits in a structured sleep protocol#
For anyone considering a personal trial, the protocol layer matters more than the peptide. The literature suggests three guardrails worth taking seriously:
- Define the problem first. DSIP's effect is concentrated in disturbed sleep. Quantify the disturbance with at least two weeks of baseline tracking (wearable, sleep diary, ideally a validated questionnaire) before introducing any compound.
- Set objective endpoints. Total sleep time, sleep efficiency, wake-after-sleep-onset, and deep-sleep percentage are all measurable. Decide in advance what magnitude of change would justify continuation and what would trigger discontinuation.
- Run a finite cycle. The animal dose-response data show non-linear effects and the human data show effects mainly in the first six hours post-injection. A four-to-six-week trial with weekly review is more informative than an open-ended habit.

How Klarovel works is built around exactly this protocol logic: curated templates, supplier connections that operate within regulatory guardrails, and an editorial layer that does not pretend the evidence is stronger than it is. The peptide calculator handles reconstitution math; the protocol library handles the rest.
For readers comparing options, the broader peptides-for-sleep overview covers other sleep-targeted compounds (Selank, Epitalon, and the growth-hormone-axis route) that hit the same endpoint of deeper slow-wave sleep through different mechanisms.
The honest summary#
DSIP is not a wonder compound, and the literature does not pretend it is. What the research has shown is a small, decades-old corpus of human data pointing to modestly improved sleep continuity, animal data demonstrating clean shifts toward deep slow-wave sleep, and a mechanistic profile that is associated with HPA-axis modulation rather than blunt sedation. The unresolved diurnal-rhythm paradox keeps DSIP firmly in the investigational column, and the FDA's immunogenicity flag is worth weighting seriously. For anyone considering a structured trial, the protocol layer (timing, dose discipline, objective sleep tracking, defined exit criteria) matters more than the peptide itself. Create a Klarovel account to access curated protocol templates, read the full disclosures, and connect with the supplier network that operates within these guardrails.
Frequently asked questions
Keep reading
Hexarelin Peptide: The Forgotten GHRP and Why It Faded
Hexarelin was once the most potent GHRP known. Research suggests tachyphylaxis and CD36 side effects explain why the peptide world moved on.

Tesofensine: The Fourth-Class Weight Loss Peptide Guide
Tesofensine is a triple monoamine reuptake inhibitor that produced 10.6% weight loss in Phase 2. Mechanism, doses, safety, and GLP-1 comparison.

Peptides for Bodybuilding: What the GH-Axis Research Shows
A clinical look at GH-axis peptides used in physique work: what the human trials on MK-677, CJC-1295 and ipamorelin actually document, plus WADA rules.